 Hereditary Leiomyomatosis and Renal Cell Cancer is a very rare genetic condition that was named in 2002. This handbook has been created to help educate and support all those impacted by HLRCC.
Hereditary Leiomyomatosis and Renal Cell Cancer is a very rare genetic condition that was named in 2002. This handbook has been created to help educate and support all those impacted by HLRCC.
Also, the HLRCC Handbook Edition 2.0 is available as paperback from Amazon (Link) and as ebook from Smashwords (Link)
Contents
Below is the online version of the HLRCC Handbook Edition PRE-3.0 – The Menu links point to the relevant section on the page. The Handbook is kept up-to-date with the latest information.
PLEASE NOTE – MRI SCREENING GUIDELINES WORDING UPDATE
Pheochromocytoma and Paraganglioma are new possible HLRCC Symptoms.
HLRCC Foundation (Formerly HLRCC Family Alliance)
Medical, Research and Support Council
Supporting the HLRCC Foundation c/o VHLA
- Diagnostic Criteria
- Genetic Testing
- Cutaneous Leiomyomas (Skin Bumps)
- Uterine Fibroids
- Renal (Kidney) Tumors
- Pheochromocytomas and Paragangliomas(Courtesy of VHL Alliance)
- Magnetic Resonance Imaging (MRI)
- Computed Tomography (CT Scan)
- Computed Tomography Photon-Counting
- Positron Emission Tomography (PET)
- Ultrasound
- Bone Scan
- Scan Contrast Agents Recommendations
SUGGESTED SCREENING GUIDELINES
- HLRCC Foundation Suggestions From Birth
- Upon HLRCC Diagnosis (At Any Age Greater Than 8)
- For Children at Risk Under 8
- Feedback – You Can Help Us Learn
- HLRCC Foundation Website
- Smart Patients
- RareConnect HLRCC Community
- INSPIRE
- VHL UK/Ireland Charity
- UK KIDNEY CANCER SUPPORT NETWORK
- Kidney Cancer Forums
- Other Sites
- The Natural History Study at the National Institutes of Health
- UCLA HLRCC Registry and Study
- Phase II Study of Pamiparib and Temozolomide
- Phase II Study of Bevacizumab and Erlotinib
- Phase I/II Study of Vandetanib and Metformin
- Phase II Trial of the DNA Methyl Transferase Inhibitor Guadecitabine (SGI-110)
- Phase I Study of the Glutaminase Inhibitor CB-839 in Solid Tumors
- Phase 2 Trial Olaparib with and without AZD1775, AZD5363, and AZD2014 in Treating Patients with Advanced Solid Tumors
- Treatment of Cutaneous Leiomyomas with Botulinum Toxin
- Intravenous Recombinant Human IL-15
EXTENSIVE LIST OF RELEVANT RESEARCH ARTICLES
BACKGROUND of the TERM “HLRCC”
HOW DO CHANGES IN DNA CAUSE CHANGES IN FUMARASE?
GLOSSARY: Definitions of Commonly Used HLRCC Terms
Family Letter (to send to relatives of someone recently diagnosed with HLRCC)
Welcome Friend
Chances are that if you are reading this page, you or someone you know has been impacted by HLRCC. We are very glad that you are here; to gather information, learn about this condition, and most importantly, to take control of your own, your patient’s, or your loved one’s health.
If you want a quick overview of HLRCC, there is a 2 page hand-out called “QUICK FACTS,” to print and keep handy.
The term HLRCC did not exist a few years ago. Other older terms for this condition are Reed’s syndrome or MCUL. Then ten years ago the connection to the possibility of developing kidney cancer and the role of the FH gene was found giving rise to the new term. Communicating to the outside world about this condition has been slow and arduous, although we are making progress. So far, up to 1000 individuals have been involved in studies regarding this condition, but most likely thousands more individuals are going undiagnosed. In our attempt to protect ourselves and our family members, those of us diagnosed with HLRCC have learned the value of annual screening. If people with HLRCC are going to stay healthy, they have to understand the risks and take action to protect themselves. These facts, along with the knowledge that most doctors do not even know that this condition exists, prompted us to create this handbook.
The purpose of the HLRCC Foundation Handbook is:
- To teach patients how to take control of their own health once they are diagnosed
- To provide medical professionals with a convenient summary of the latest information available on HLRCC, and how best to manage the health of a patient with HLRCC.
- To communicate the importance of both screening for kidney tumors and conducting genetic testing for blood-related family members
- To offer doctors and patients resources for clinical research, tips for efficient and safe screening, and the most up-to-date information possible regarding current research and statistics for HLRCC
Finally, it is our hope that the HLRCC Foundation through its web site, Facebook Group, and this handbook will provide you with emotional support. An additional online resource is Inspire where those impacted by HLRCC, VHL, and BHD can exchange information, stories and encouraging words. We encourage you to join and partake. They are wonderful resources!
Thank you for your support and for doing all you can to spread the word about HLRCC. Remember, KNOWLEDGE SAVES.
Warmly,
Julie Haff Rejman, Chair
Hereditary Leiomyomatosis and Renal Cell Cancer (HLRCC) Foundation
c/o VHL Alliance
1208 VFW Parkway // Suite 303
Boston, MA 02132 USA
Tel: +1 800 767-4845 ext. 709 (toll-free) or +1 617 277-5667 ext. 709
Fax: +1 866-209-0288 (toll-free) or +1 858-712-8712
Email: admin@hlrccinfo.org
The HLRCC Foundation is indebted to the VHL Alliance for their generous financial and administrative support. Although the HLRCC syndrome is not linked to von Hippel-Lindau (VHL), or Birt-Hogg-Dubé (BHD) they are all related on the path to kidney cancer, and the three syndromes have a number of common characteristics.
See https://www.vhl.org/ and https://www.bhdsyndrome.org/
HLRCC Foundation (Formerly HLRCC Family Alliance)
At the urging of Lindsay Middelton, Genetic Counselor at the US-NCI, and with the support of Joyce Graff of the then VHL Family Alliance, (Now VHL Alliance), Phil Thayer founded the HLRCCF in the autumn of 2004 and continued as leader of the group until early 2011. Key Milestones
In February 2011, Julie Haff Rejman became the Chair of the organization. Graham Lovitt became the Vice Chair.
In January 2013, Antony Horton Ph.D., also became a Vice-Chair.
In December 2022, Bruce Lee one of our Vice-Chairs and Driven To Cure CEO sadly died.
In March 2023, The rebranded HLRCC Foundation was defined.
HLRCC Foundation Board of Director
President: Dean Elhag, USA
Vice-President: Jason DiCola, USA
Secretary: TBA
Treasurer: TBA
Joshua Mann,MPH., Director of Engagement and Outreach, VHL Alliance, USA
Antony Horton, Ph.D.,Vice Chair HLRCC Foundation, previously Chief Scientific Officer at the International Rett Syndrome Foundation,
Website/Social Media Lead: TBA
HLRCC Foundation Board of Trustees
Chair: Julie Haff Rejman, Colorado, USA
Vice-Chair: Antony Horton Ph.D., UK
Vice-Chair: Graham J Lovitt, UK
Vice-Chair: Jo Parker
Vice-Chair: Vittoria Rollo, Italy
Powerful Patient: Joyce Graff, M.A., Massachusetts, USA
- HANDBOOK CO-AUTHORS:
Joyce Graff, Graham Lovitt, Julie Haff Rejman, and Alison Smith - HANDBOOK CONTRIBUTORS AND REVIEWERS:
Julie Adam, Ph.D., Lindsay Middelton, Pamela Stratton, M.D., and Ian Tomlinson, Ph.D. - WEBSITE SUPPORT and DESIGN:
Website designer: Angela Render Original logo design: Dr. Daniel Rejman DDS, MS
Digital logo graphic: Ingrid Morris
Privacy Policy
The HLRCC Foundation website previously subscribed to the principles of HONcode of the international Health on Net Foundation, to assure you of the highest quality of health information.
Medical information on this site is reviewed by our Medical, Research and Support Council.
Information provided on the website is designed to support, not replace, the relationship that exists between a patient or site visitor and his or her physician.
The website does not accept advertising. It is supported solely by donations from people with HLRCC, their friends, their families and supporters, and physicians and researchers interested in HLRCC.
Privacy
Personal details that you provide to the HLRCC Foundation, including e-mail addresses, are kept entirely confidential. These details are shared within this organization among staff and volunteers for the purpose of providing service to you, but are never shared with, rented or sold to other organizations. All staff and volunteers have made confidentiality agreements to protect your information. To verify your information or send corrections, please contact us at admin@hlrccinfo.org
Information you submit to us voluntarily through the website is stored on our secure server using SSL encryption technology.
Computer Tracking and Cookies
The website is not set up to track, collect or distribute personal information not entered by visitors. Our site logs do generate certain kinds of non-identifying site usage data, such as the number of hits and visits to our sites. This information is used for internal purposes by technical support staff to provide better services to the public and may also be provided to others, but again, the statistics contain no personal information and cannot be used to gather such information.
The website also recognizes the online site where a visitor searched to find a subject which brought them to the HLRCCF website, but we cannot identify the visitor or the visitor’s address. Site information is used to help us serve these search sites with the correct information about our material. No personal information is collected.
A cookie is a small amount of data that is sent to your browser from a Web server and stored on your computer’s hard drive. HLRCCF does not use cookies in its web pages. We do not generate personal data, do not read personal data from your machine and do not store any information other than what you voluntarily submit to us.
Problems or Complaints with HLRCCF Privacy Policy
If you have a complaint about HLRCCF compliance with this privacy policy, you may contact us at admin@hlrccinfo.org.
Links to Third Party Sites
The links included within the service may let you leave this site. The linked sites are not under the control of HLRCC Foundation and HLRCCF is not responsible for the contents of any linked site, or any link contained in a linked site, or any changes or updates to such sites. These links are provided as a convenience only, and the inclusion of any link does not imply endorsement by HLRCCF of the site or any association with their operators.
If you have technical questions about this site, please contact: admin@hlrccinfo.org.
Medical, Research and Support Council
Current Members
Julie Adam, Ph.D., Researcher, Nuffield Department of Medicine, Oxford, UK
Kristiina Aittomäki, M.D., Ph.D., Professor, Head of the Department of Clinical Genetics, HUSLAB ,Helsinki University Hospital, Finland
Gennady Bratslavsky, M.D., Chair of Urology, Upstate Medical Center, Syracuse, NY, USA
Patrick R. Carrington, M.D., Dermatologist and Associate Editor of the Journal of the American Academy of Dermatology, Greenwood Village, CO, USA
Carlos Alberto Fredes, Executive Director of the Argentina Association of Families of Von Hippel-Lindau (VHL-AAF) Argentina
Eyal Gottlieb, BSc., MSc., Ph.D., Research Group Leader, Beatson Institute of Cancer Research, Glasgow, Scotland, UK
Joyce Graff, M.A., Powerful Patient, Inc., Massachusetts, USA
Antony Horton, Ph.D.,Vice Chair HLRCC Foundation, previously Chief Scientific Officer at the International Rett Syndrome Foundation, founder and C.E.O. of his own small company PharCited, which provides strategic advice to the biomedical non-profit sector, New York, USA
W. Marston Linehan, M.D., Chief, Urologic Oncology Branch, National Cancer Institute*, USA
Graham J. Lovitt, Vice Chair HLRCC Foundation, retired software quality assurance manager, software systems designer, UK
Eamonn R. Maher, M.D., FRCP, FMedSci, Professor of Medical Genetics and Genomic Medicine, University of Cambridge, UK
Joshua Mann,MPH., Director of Engagement and Outreach, VHL Alliance, USA
Fred H. Menko, M.D., Ph.D., Consultant Clinical Geneticist, VU University, Amsterdam, The Netherlands
James W. Mier, M.D., Associate Professor, Department of Medicine, Harvard Medical School, USA
Julie H. Rejman, MSW, Chair of HLRCC Foundation Board, Castle Rock, CO, USA
Stéphane Richard, M.D., Ph.D., Professor of Oncogenetics and Chair, National Expert Centre for Rare Cancers PREDIR, Le Kremlin-Bicêtre, France
Laura S. Schmidt, Ph.D., Urologic Oncology Branch, National Cancer Institute*, USA
Pamela Stratton, M.D., Gynecologist, National Institute of Child Health and Human Development, US-NIH,Bethesda, MD, USA
Sunil Sudarshan, M.D., Assistant Professor UTHSCSA, Urology, San Antonio, TX, USA
Min-Han Tan, MBBS FRCP FAMS PhD, CEO and Medical Director of Lucence Diagnostics Pte Ltd.
Ian Tomlinson, BA MA Ph.D. Camb, BM Brist, BM BCh Oxf, Professor of Molecular and Population Genetics, Nuffield Department of Medicine Oxford, UK
Jorge R. Toro, M.D., Investigator, Dermatology Branch, National Cancer Institute*, USA
Ingrid Winship, MB ChB, MD, FRACP, FACD., Professor of Adult Clinical Genetics, University of Melbourne and Royal Melbourne Hospital, Melbourne, Australia
*The National Cancer Institute (US-NCI) is one of the National Institutes of Health (US-NIH), Bethesda, MD, USA
Honorary Members
Although no longer actively involved, in recognition of their contribution to the world of HLRCC the following have kindly agreed to be listed.
- Virpi Launonen, Finland, Author of the paper establishing the connection between symptoms of HLRCC and the gene on chromosome 1 (2001)
- Phil Thayer, USA, Founder of HLRCC Family Alliance in 2004
R.I.P. Bruce H. Lee, Founder with Andrew Lee of Driven to Cure
Supporting the HLRCC Foundation c/o VHLA
The original HLRCC Family Alliance was founded in 2004 as a support group for people affected by Hereditary Leiomyomatosis and Renal Cell Cancer and interested health care professionals, and to promote research. Funding the VHL Alliance helps support our website and any outreach we do to the medical community, including such things as domestic and international mailings, attending medical conferences related to HLRCC, or supporting travel expenses for HLRCC educators. The VHL Alliance is funded by the generosity of its supporters. The HLRCC Fouudation is currently not a separate legal entity and is kindly supported by VHL Alliance infrastructure. It is intended for the HLRCC Foundation to become a non-profit charity with the tax authorities in the United States.
* The VHL Alliance is registered as a non-profit charity with the tax authorities in the United States, Canada, and Great Britain, as well as other countries. Please contact your local group and your tax advisor for specific information on guidelines for tax deductibility of donations.
Please mail the following Supporter/Donation form to HLRCC Foundationc/o VHL Alliance, 1208 VFW Parkway // Suite 303, Boston, MA 02132 USA. Thank you!
Supporter/Donation Form
Download the Supporter/Donation form.
QUICK FACTS
Download the Quick Facts for your convenience.
- HLRCC stands for Hereditary Leiomyomatosis and Renal Cell Cancer (sometimes Carcinoma). It is also known as Reed’s Syndrome (legacy term).
- HLRCC is caused by an inherited genetic alteration in the Fumarate Hydratase (FH) gene. There is a 50% risk of passing this on and the severity of the disease can vary a lot from person to person. It can be diagnosed by the detection of this genetic alteration (mutation).
- Many women with HLRCC develop large uterine fibroids in their twenties. Although benign, the fibroids may result in early treatment.
- Both men and women tend to develop benign skin leiomyomas (or “skin bumps”) in their twenties. These two symptoms together, fibroids and skin leiomyomas, offer an important clue to the need for genetic testing of the FH gene. Because of the absence of uterine fibroids, HLRCC is more likely to go undetected in men, and early diagnosis is less likely.
- Screening requires an annual MRI scan of the abdomen for the detection of kidney cancer. The MRI scan for HLRCC patients should use pre-and post- contrast 3D acquisition with as high a resolution as possible, 3mm or less slice reconstruction is advised. Clinicians at the National Institutes of Health are currently using 1mm slice reconstruction in this population. The scans should be reviewed by someone with expert HLRCC knowledge especially if kidneys cysts are present. Be sure to read the Handbook section “Suggested Screening Guidelines” for more information.
- Even small HLRCC kidney tumors can metastasize, or spread, very quickly to the bones, lungs and brain. Unlike some other cancers, there is no curative treatment for kidney cancer once it metastasizes, although life may be extended with the latest class of drugs. Annual screening helps our goal to prevent metastasis and to stay healthy.
- If you live in the United States, you may want to consider being part of a clinical trial at the National Institutes of Health (US-NIH) in Bethesda, MD. This is the only trial open at the time of writing. We expect that more will be opened in the future, possibly at other locations around the world.
- It is recommended that children who have a parent with HLRCC have genetic testing by age 8 as screening is recommended from that age for children at risk. Please read more about this in the Handbook..
- It is a newly identified condition (2002) and is currently being studied at several locations around the world.
- There are approximately 200-300 families currently diagnosed with HLRCC with perhaps 1500 patients. It is an under-diagnosed condition because of its rarity.
- Being diagnosed with HLRCC can be a very scary thing, mostly because it has the word cancer in its heading. If you have HLRCC it does not mean that you have kidney cancer or will necessarily get it. However it does mean that you have an increased risk factor for kidney cancer, and you need to screen yourself so that doctors can detect even the smallest HLRCC cancer in your kidneys.
- Our motto is Knowledge Saves. Although it is sometimes difficult to come to terms with a new diagnosis, we provide you and your family with information to protect yourselves and future generations. Knowledge truly is a gift.
- We encourage you to look through our website and the handbook. We also encourage you to reach out to us and ask for support – or offer it to another member. We are a small group, but we are very active, even on Facebook! We hope you will join us!
- https://www.hlrccinfo.org
- https://vhl.inspire.com
- Rare Connect HLRCC Community
- HLRCC Foundation Facebook Private Group
- HLRCC Foundation Facebook Page
- The HLRCC Foundation 1-800-767-4845 extension 709
- HLRCC Foundation c/o VHL Alliance, 1208 VFW Parkway // Suite 303, Boston, MA 02132 USA.
Enjoy this beautiful day!
AN OVERVIEW: What is HLRCC?
In recent years, scientists have used the work of the Genome Project to help identify new connections between physical symptoms that used to be viewed as isolated or random. One of these diseases is called HLRCC, or Hereditary Leiomyomatosis and Renal Cell Cancer. HLRCC is a rare inherited condition first fully described in 2001. It is caused by a tiny alteration in one copy of the FH gene.
According to researchers at the US-NIH HLRCC is a rare inherited condition characterized by the presence of cutaneous leiomyomas, uterine fibroids, and/or kidney cancer. A person who is diagnosed with HLRCC has inherited a susceptibility to develop one or more of these symptoms.
Approximately 450 people have been evaluated at the US-NIH, along with many other people in England, France, Japan, Finland, and Australia, but it is believed that there are many more people who are undiagnosed. Considering HLRCC is a relatively new, and rare condition, there remains much to be learned.
There is considerable variation in symptoms from family to family and among members of the same family. Each person in a family has their own individual susceptibility to the symptoms. For example, if your parent had kidney cancer, it does not mean you will develop a kidney tumor. You have your own unique susceptibility.
Even if a child inherits the altered gene, it does not necessarily mean that he or she will have any symptoms of HLRCC. There may never be any symptoms at all. Or that person may develop just one of the issues, or two, or possibly all three. So far, researchers have not been able to find any patterns that would allow one to predict which symptoms a person will develop based on the particular genotype they have. However, there do seem to be trends in some families. Some families seem to only get leiomyomatosis and other families are more likely to get RCC (kidney cancer).
HLRCC is caused by having an alteration (mutation) in one copy of the Fumarate Hydratase (FH) gene. The FH gene is a section of DNA that codes for a protein called fumarase. Fumarase is an important enzyme needed for the production of energy by mitochondria, which are the tiny organelles inside our cells that produce most of our cells’ energy. All people have fumarase and researchers are trying to learn the normal function of fumarase and why alterations in the FH gene cause the symptoms of HLRCC.
HLRCC is inherited in an Autosomal Dominant manner, meaning that both males and females can be affected, and each child of an affected parent has a 50% chance of inheriting the altered FH gene.
All people have two copies of the Fumarate Hydratase gene, one from their mother and one from their father. In a person with the condition called HLRCC, one of their two genes is normal and working well. The other is altered, meaning that it has a change in it and does not work very well. The altered FH gene is unable to produce the fumarase enzyme properly. When a person has only one working copy of the gene, their cells make less fumarase than normal, but enough to be healthy. During a person’s lifetime, genes can become damaged when alterations occur during cell division or from exposure to chemicals or radiation. Cells have the ability to repair damaged DNA, but sometimes they cannot, leaving a non-working altered gene in a cell. In a person with HLRCC, an alteration in the second copy of the FH gene can lead to biochemical changes that cause those cells to grow into benign smooth muscle tumors (leiomyomas) of the skin and uterus, or less often malignant tumors of the kidney. For more detailed information regarding the FH enzyme, please refer to our HLRCC Science.
Diagnostic Criteria
Although there is no consensus on diagnostic criteria, the US-NIH and other experts believe that an individual has HLRCC if they have any of the major features of the condition, including:
Cutaneous leiomyomas: Most individuals with HLRCC present with multiple cutaneous leiomyomas (skin bumps). A single cutaneous leiomyoma on its own is insufficient to confirm an HLRCC diagnosis unless another family member has already an HLRCC diagnosis. However, continuing to be vigilant and possibly having a single baseline MRI scan of the kidneys should be followed.
Uterine Leiomyomas: Most females with HLRCC have uterine fibroids, often quite large and occurring early in their 20s. However, fibroids are very common in the general population and are rarely diagnostically useful on their own.
Kidney (Renal) tumors: Most people who have HLRCC do not develop kidney tumors. The incidence of kidney tumors in the US-NIH study group is about 30%. However, the incidence of kidney tumors in the European group is reported as much lower. We are still learning the specific factors that increase or decrease one’s risk of kidney cancer.
A positive genetic test for HLRCC: This means that an alteration has been detected in the Fumarate Hydratase gene. FH alterations can be found in about 97% of families who are strongly suspected of having HLRCC.
If HLRCC is suspected, but the genetic alteration cannot be found and there are no cutaneous leiomyomas, then a fumarase enzyme assay can be done on cells derived from skin or blood. A fumarase activity level less than or equal to 60% is indicative of HLRCC. This test is specialized and it is not available in most laboratories. Some laboratories that can test for fumarase activity find difficulties because of problems in calculating and interpreting the results.
Recently some pheochromocytomas and paragangliomas have been found to be associated with HLRCC and there is now a new section added to this Handbook.
There are other cancers which have been occasionally associated with HLRCC. Breast and prostate are examples. Some HLRCC family members have other health problems (an example is thyroid nodules), but it is not clear if these are related to HLRCC. At this point they are assumed to be coincidental. We are all still members of the general population.
Note: Researchers in England discovered a difference between HLRCC tumors and non-HLRCC tumors (kidney and other tumors). This is called the immunohistochemistry for 2-Succinocysteine (2SC) test. Fumarase deficient cells give positive staining meaning that the cells are HLRCC positive.
Note: There are other tumor types where the number of cases is too small to allow us to categorize these tumors as diagnostic criteria for HLRCC, but when they occur in an HLRCC patient, the tumors are found to have no fumarase activity. Examples are benign adrenal tumors and Leydig testicular cancer which develops in the Leydig cells — the cells in the testes that release the male hormone, testosterone. There is also a possibility of benign ovarian cystadenomas and some Wilms’ tumors being associated with HLRCC.
Although there is no consensus on diagnostic criteria, the US-NIH and other experts believe that an individual has HLRCC if they have any of the major features of the condition, including:
Cutaneous leiomyomas: Most individuals with HLRCC present with multiple cutaneous leiomyomas (skin bumps).
Uterine Leiomyomas: Most females with HLRCC have uterine fibroids, often quite large and occurring early in their 20s. However, fibroids are very common in the general population and are rarely diagnostically useful on their own.
Kidney (Renal) tumors: Most people who have HLRCC do not develop kidney tumors. The incidence of kidney tumors in the US-NIH study group is about 30%. However, the incidence of kidney tumors in the European group is reported as much lower. We are still learning the specific factors that increase or decrease one’s risk of kidney cancer.
A positive genetic test for HLRCC: This means that an alteration has been detected in the Fumarate Hydratase gene. FH alterations can be found in about 97% of families who are strongly suspected of having HLRCC. 2024 – FH alterations are now termed variants and are classified into Pathogenic, Likely Pathogenic, Variant of Uncertain Significance VUS, Likely Benign, and Benign. see the ClinVar database. If your variant is not defined as Pathogenic or Likely Pathogenic there may be problems in getting screening costs covered and having procedures like Pre-implantation genetic testing for monogenic disorders (PGT-M) – Previously Pre-implantation genetic diagnosis (PGD).
If HLRCC is suspected, but the genetic alteration cannot be found and there are no cutaneous leiomyomas, then a fumarase enzyme assay can be done on cells derived from skin or blood. A fumarase activity level less than or equal to 60% is indicative of HLRCC. This test is specialized and it is not available in most laboratories. Some laboratories that can test for fumarase activity find difficulties because of problems in calculating and interpreting the results.
Recently some pheochromocytomas and paragangliomas have been found to be associated with HLRCC and there is now a new section added to this Handbook.
There are other cancers which have been occasionally associated with HLRCC. Breast and prostate are examples. Some HLRCC family members have other health problems (an example is thyroid nodules), but it is not clear if these are related to HLRCC. At this point they are assumed to be coincidental. We are all still members of the general population.
Note: Researchers in England have discovered a chemical compound that is present in HLRCC tumors, but not in non HLRCC tumors (kidney and other tumors), so in the future we may see newer and better screening tests for HLRCC.
Note: There are other tumor types where the number of cases is too small to allow us to categorize these tumors as diagnostic criteria for HLRCC, but when they occur in an HLRCC patient, the tumors are found to have no fumarase activity. Examples are benign adrenal tumors and Leydig testicular cancer which develops in the Leydig cells — the cells in the testes that release the male hormone, testosterone. There is also a possibility of benign ovarian cystadenomas and some Wilms’ tumors being associated with HLRCC.
Genetic Testing
HLRCC is an autosomal dominant disorder. “Autosomal” means that the alteration is located on one of the 22 regular chromosomes and not on a sex chromosome (X or Y). “Dominant” means that having just one copy of the altered gene is enough to cause the disorder. This means that if a person has HLRCC, there is a 50% chance that he or she will pass the altered gene to a child. There is a 50% chance that an embryo of an HLRCC parent will have the condition, depending on whether the particular egg or sperm from which that the embryo was formed contained the altered copy of the gene. You have two FH genes – one from each parent. The one healthy parent gives you one healthy unaltered FH gene. The other parent with the altered gene gives you one of their two copies of the gene: either a healthy unaltered FH gene or an altered FH gene – hence the 50% chance. You either have an altered gene or you don’t. Occasionally a person with an altered FH gene may have very few symptoms, so that it may seem to skip a generation, but if you do not have an altered FH gene you cannot pass it to a child. It is possible for an alteration in the FH gene to be present for the first time in one family member as a result of a mutation in a germ cell (egg or sperm) of one of the parents or in the fertilized egg itself. This is termed a “de novo mutation”.
|
|
Parent 2 without HLRCC |
Each child gets one copy of the FH gene from each parent.
In this way, there are four possible arrangements of these four genes. Each arrangement has a 25% chance.
So for each child there is a 50% chance of having HLRCC and a 50% chance of not having it.
 AC: Child AC: ChildWith HLRCC A=FH Gene Mutation C=FH Working Gene |
AD:Child With HLRCC A=FH Gene Mutation D=FH Working Gene |

BC: Child |
BD: Child |
Genetic testing is the most reliable way of diagnosing HLRCC. Although a physician can often diagnose an individual with HLRCC based on the physical signs listed above, the US-NIH recommend that individuals obtain genetic testing to confirm that they actually have the gene alteration.
Benefits of genetic testing to confirm HLRCC:
- A positive test (meaning you do have HLRCC) will help people advocate with their doctors and insurance companies for agreement with their need for annual kidney screening.
- It gives family members who do not have symptoms the ability to discover whether they have the gene alteration by a simple blood test.
- A negative test (meaning you do not have HLRCC) can put your own fears to rest when other family members have tested positive (meaning they have HLRCC).
- As we learn more, the exact alteration in your gene will become increasingly important to your own health maintenance.
Things to keep in mind regarding genetic testing:
- It may complicate your ability to obtain life or health insurance. Refer to section about Life and Health insurance. Genetic testing and lifetime kidney surveillance is expensive. It is much easier if a person has health insurance in place before obtaining a DNA test.
- It can be an emotional process. It is not a simple blood test. The results may be difficult to interpret, and it is best to undertake genetic testing through a genetic professional (geneticist or genetic counselor) who can help you understand the results and their implications for yourself and your family.
- If you have your children tested before their age of consent and they are found positive there are implications for future life or health insurance, and mortgage applications as well as the start of a life-long screening process. This is a difficult decision to make between health safety and financial implications. We recommend that people have life insurance in place even for children before obtaining a DNA test. Many countries are passing anti-discrimination laws to protect citizens.
If you are in the worldwide HLRCC clinical study at the US-NIH (Bethesda, Maryland, USA):
- Genetic testing at US-NIH is optional, so you can still be in the study and not have the genetic testing done. This is especially beneficial if you have physical signs and family members who have had positive genetic testing, but don’t want the testing done yourself. All testing at US-NIH is optional.
If you are not in the US-NIH study, you should look for a genetic counselor from your area online. The best links to use are:
US – https://www.nsgc.org/
World – https://geneclinics.org and go to the link for Clinic Directory
You will want to bring a copy of a clinical paper about HLRCC such as the Toro article https://www.ncbi.nlm.nih.gov/books/NBK1252/ with you to your genetic counselor and your genetic counselor is welcome to contact Lindsay Middelton at US-NIH or another expert consultant to obtain further information. You should also give your genetic counselor the link www.hlrccinfo.org so that they can make sure you get the screening you need when they connect you with the proper physicians, should your test be positive.
References:
- Pithukpakorn M, Toro JR., Hereditary Leiomyomatosis and Renal Cell Cancer. GeneReviews [Internet]. 2010. PMID: 20301430,
https://www.ncbi.nlm.nih.gov/pubmed/20301430
https://www.ncbi.nlm.nih.gov/books/NBK1252/
The risk of developing the features of HLRCC increases with age. You are at significant risk of being diagnosed with an FH gene alteration if you have a diagnosed blood relative. The actual risk figure depends on the closeness of the relationship starting as high as 50% with a first degree relative (parent, child or sibling). There is a lower risk of 25% with a second degree relative (uncle/aunt, niece/nephew or a grandparent) and a still lower risk with a third degree relative (first cousin) or even a first cousin’s child. The alteration cannot however skip generations so the more genetic testing a family has the more precise the risk figure will be for each individual ranging from 0% to 50%. In other words, if one of your parents is at risk, but tests negative, then you will not be at risk. If a person does not carry the altered gene, they cannot pass it to a child. You may wish to discuss this with your genetic counselor for more clarification.
If you test positive and want to inform other family members, there is at the end of the handbook, a printable Family Letter (to send to relatives of someone recently diagnosed with HLRCC). The letter should only come from the person with the HLRCC diagnosis, or the next-of-kin if the person has died, in order to respect their privacy. It is important to keep in mind that your family members may be overwhelmed when they receive this information. We tried to keep this in mind when creating our printable letter and to offer the support of the HLRCC Foundation as a way of supporting each and every person associated with this condition.
If your genetic test is negative, but you have symptoms of HLRCC you should check that your genetic test covered the possibility of FH deletions including whole gene deletion, in addition to bidirectional sequencing. This is usually through a technique called MLPA or multiplex ligation probe amplification. Some companies only offer sequencing.
It can sometimes take several months to obtain genetic testing results, but once one genetic alteration is identified within the family, testing of additional family members is faster and less costly. Tests in some countries are faster than others. Please consider the following PROS and CONS when considering genetic testing as well:
PROS:
-
- Knowing about the HLRCC genetic alteration gives you the insight to screen and protect yourself or your siblings/children or other family members, if they are tested. Knowledge is power!
- Catching HLRCC tumors early may save your life. A kidney tumor often grows with no symptoms. Periodic screening with scans will catch a tumor early, so that it can be treated.
CONS:
- A positive test result may have an impact on your own and your children’s ability to get life or health insurance. You should be sure to have coverage before requesting DNA testing.
- The knowledge of a condition such as this has emotional implications. People can become very worried about the future, which is where a support group such as HLRCC Foundation www.hlrccinfo.org can help to put your life back on track.
Life and Health Insurance
A useful link describing the general implications for insurance (applies to all genetic conditions not just to Birt-Hogg-Dubé) ishttps://www.bhdsyndrome.org/for-families/additional-resources/insurance/ and there is information for different US States in https://www.healthinsuranceinfo.net/
Concerns about Genetic Discrimination of Health Insurers
Many people who learn they may have HLRCC are concerned that their health insurance company will either terminate their policy or deny coverage if the insurer learns of their genetic status. Many states have enacted state laws to protect their citizens from genetic discrimination by health insurers. However, the protection offered varies widely among state laws. You can access information about your state law by accessing: https://genome.gov > Issues in Genetics > Statute and Legislation Database https://www.genome.gov/PolicyEthics/LegDatabase/pubsearch.cfm
In 2008 the Genetic Information Nondiscrimination Act (GINA) was signed into law. The GINA Act prohibits discrimination by health insurance companies and employers based on “genetic information”, including information about genetic testing or your results (and those of your family members) or information about family history of any disease or disorder.
Health insurance protection:
- Group and individual health insurers may not use your genetic information to set eligibility, premium or contribution amounts;
- Health insurers may not request or require that you take a genetic test.
Employment protection:
- Employers may not use your genetic information to make decisions involving hiring, firing, job assignments and promotions;
- Employers may not request, require or purchase genetic information about you or one of your family members. GINA stipulates that genetic information alone cannot be considered a pre-existing condition.
What does GINA NOT do?
- GINA does NOT restrict health care providers from requesting, offering or providing information about a genetic test to patients.
- GINA does NOT require insurance companies to pay for any particular test.
- GINA does NOT apply to life, disability or long term insurance.
- If you have been diagnosed with a medical problem or a symptom related to HLRCC, GINA does NOT apply
Employers with fewer than 15 employees and the military are not required to abide by the employment protections.
Having Children
Deciding whether to have children when there is a 50% chance of inheriting a problem is a difficult decision to make. Before making any decision you may wish to speak with a geneticist or genetic counselor about possible testing options and its implications. One option may be Pre-implantation Genetic Diagnosis (PGD). There is information on the VHL Alliance website about PGD. See https://www.vhl.org and also “Family planning with VHL, HLRCC and BHD – what you need to know”
Other options may include Chorionic Villus Sampling (CVS) or amniocentesis.
It’s advisable for the other non-HLRCC parent to be genetically tested for any FH Gene variant that is known to be pathological for Fumarase Deficiency to avoid the possibility of having a Fumarase Deficient child.
Cutaneous Leiomyomas (Skin Bumps)
There is considerable variation in the appearance of cutaneous leiomyomas as can be seen in the following photographs making it difficult to diagnose by sight unless you are a specialist.




Photos 2, 3 and 4 courtesy of Dr. Ed Cowen, NIH, NCI.
Just as uterine leiomyomas grow from smooth muscle of the uterus, cutaneous leiomyomas are rare benign tumors that grow from smooth muscles in the skin. The arrectores pilorum (singular arrector pili, also called piloerectus muscles) are small smooth muscles that are attached to hair follicles. These are the muscles that allow your hairs to “stand up” when you are cold or fearful. When benign tumors grow from arrrectores pilorum, they are called piloleiomyomas. They also may be called cutaneous leiomyomas. It is estimated that most people with HLRCC will get one or more piloleiomyomas in their lifetime.
Piloleiomyomas are very helpful for identifying people who are likely to have HLRCC.
Individuals who have HLRCC tend to have cutaneous leiomyomas by the time they are in their 30’s, but some have gotten them as early as 11 years old; some people report finding their first one in their 50’s.They tend to grow anywhere on the body and limbs, but rarely on the face, hands or feet. These bumps can be very small, but sometimes large, can range in color from skin-colored to light brown to red, and tend to grow in mosaic clusters, but can also be solitary. Some people have a single leiomyoma, but many people develop small clusters of leiomyomas. A smaller percentage of people develop wide distribution of leiomyomas over their chests or backs (“segmental distribution”). Once a leiomyoma appears, it does not go away.
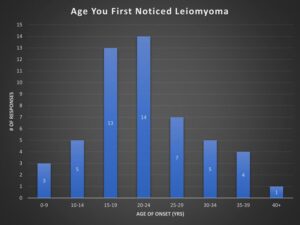
A survey taken in the HLRCC Foundation’s Facebook Group shows the onset age of cutaneous leiomyoma in a sample size of 53 members.
Leiomyomas can be mistaken for post-acne scarring. They are very firm to the touch and discrete as compared to acne or eczema. They are not common skin lesions in the general population, but dermatologists are starting to recognize them more easily as potential indicators of HLRCC.
Diagnosis
A skin biopsy must be done to confirm a leiomyoma, as relying on appearance is inconclusive. A skin biopsy involves minor surgical removal of some of the skin bump, after which the tissue is sent to a pathology lab. An anesthetic agent is injected under the skin around the leiomyoma and once the area is numb, a small sample of tissue is taken. Slides are prepared from the tissue and examined under a microscope by a pathologist to determine whether the diagnosis is piloleiomyoma or some other type of growth. This is a technical description: The smooth muscle fibers are fusiform and are composed of eosinophilic cytoplasm with elongated blunt-ended (spindle shaped) nuclei and perinuclear halos in cross-sections. Cutaneous leiomyomas are clinically very similar to other lesions and require a biopsy and histologic evaluation for confirmation. The clinical differential diagnosis includes nevus, dermatofibroma, neurofibroma, glomus tumor, angiolipoma, and other benign growths, hamartomas or neoplastic lesions. The immunohistochemistry for 2-Succinocysteine (2SC) test can be used on the removed tissue to give a precise diagnosis.
Cutaneous leiomyomas can be the only clue to a physician about whether a person is at risk for HLRCC. If one has a first-degree relative with HLRCC, then a single confirmed cutaneous leiomyoma is sufficient for the diagnosis of HLRCC. Without a first-degree relative with HLRCC at least two are required for a HLRCC diagnosis.
Pain
As with all the conditions associated with HLRCC there is considerable variation not only in the appearance of cutaneous leiomyomas, but also in the experience of pain in them. The exact cause of pain has not been understood, but there is a thought that the leiomyoma has trapped nerve cells. The variation is not just from patient to patient, but also within one patient and can increase over time. Some patients find a cold sensitivity to such an extent that they even consider moving to a warmer country. Some find that if a pain develops in one leiomyoma it acts as a trigger to all the others to become also painful for hours or days at a time. Sometimes a leiomyoma that grows initially without having any pain symptom can start to become irritable and painful. Pain can sometimes occur as a result of exertion, or by touch or rubbing clothes. When pain does occur most patients describe it as excruciating, like having a knifepoint stab.
Treatment
Cutaneous leiomyomas are often sensitive to cold and touch, but many people do not find them painful. However, in some people leiomyomas are very painful. Most dermatologists do NOT recommend surgically removing all these growths, except as needed for biopsies, as it tends to cause scarring and divots in the skin where the procedure is performed. However painful or unsightly leiomyomas, if there are not too many close together, can be surgically removed using CO2 laser or freezing with cryosurgery. Preferably the removal is by a skilled plastic surgeon to minimize scarring. Use of a super-fine thread avoids the dots on either side of the line of surgery. Removal will normally be done under a local anesthetic. There is a reported case of extensive multiple piloleiomyomas being successfully removed by surgery and reconstructed with a flap technique. Sometimes the leiomyomas will grow back after removal, possibly because some tissue was left behind, or there were new ones growing when in a cluster. You should talk with a dermatologist about what is best for your type of skin growth.
Some of our members have reported (2021) improvement by taking Vitamin D3. The maximum recommended dose is 4,000 i.u. and to help absorption of Vitamin D take with Vitamin K2 100μg (available in combined form). As always you should consult with your medical practitioner.
Researchers at US-NIH experimented with Botox therapy to help with the pain (see Clinical Trials) but there was no improvement. If you have painful cutaneous leiomyomas, you may want to get a contact name from info@hlrccinfo.org or talk with your own dermatologist about options.
One of our members has found significant relief using Lyrica. As with any treatment you should first discuss and agree its suitability with your physician and or dermatologist. The links below have a lot of information about Lyrica including descriptions of warnings and side effects which seem important to study before deciding to take it.
https://www.lyrica.com/PHN/phn-introduction.aspx and https://arthritis.about.com/od/pregabalin/a/Lyrica.htm and https://en.wikipedia.org/wiki/Pregabalin
Another pain relief drug that is being used is niphediprine. As with the use of all drugs you should consult with your medical team – especially so if intending to become pregnant.
Significant pain relief has also been reported with pulsed hysocine butyl bromide see https://www.ncbi.nlm.nih.gov/pubmed/20049277. This article mentions many calcium channel blockers like nifedipine, phenoxybenzamine, doxazocine, gabapentin and topical 9% hyoscine hydrobromide.

Courtesy of Ryan N, HLRCC patient – showing significant growing back after 3 years.
A dermatologist should conduct an annual inspection of all cutaneous leiomyomas to detect changes which might lead to malignant cutaneous leiomyosarcoma (which is a rare cancer, but may be 2% in HLRCC see paper “Reassessing the clinical spectrum associated with hereditary leiomyomatosis and renal cell carcinoma syndrome in French FH mutation carriers”).
There has been one reported case of a solitary angioleiomyoma with multiple piloleiomyomas see https://www.ncbi.nlm.nih.gov/pubmed/10356411.
Uterine Fibroids
Like the skin, the uterus contains smooth muscle tissue, and uterine fibroids are smooth muscle tumors that grow in the wall of the uterus or womb,(myometrium) and with the ligament of the womb. They are almost always benign (non-cancerous) and can be as small as an apple seed or as large as a grapefruit. Other medical terms for fibroids are myoma fibromyoma leiofibromyoma fibroleiomyoma and fibroma (the dual of myoma is myomas or myomata).
In the general population, up to 80% of women develop uterine fibroids by the age of 50 years. Uterine fibroids are the leading reason for hysterectomies in the United States (1 in 3 have fibroids). Women with fibroids may be at greater risk of having a cesarean section when they give birth. Other women with fibroids may have difficulty becoming pregnant or carrying a pregnancy. More often fibroids are simply “innocent bystanders” during pregnancy and cause no problems at all.
Uterine fibroids are often the first physical symptom to develop in a female who has HLRCC. Although a nuisance, they provide a clue to individuals who are at risk, as well as a warning to be looking for skin leiomyomas, which are often the second physical symptoms of HLRCC.
The growth of uterine fibroids is believed to be affected by hormones (byespecially the female hormones estrogen and progesterone). The occurrence of fibroids is genetic. Uterine fibroids that are associated with HLRCC tend to be larger and to occur at earlier ages than in the general population.
If you are planning to have children, it may be better to have them in your 20’s rather than to wait until your 30’s, as over time fibroids may begin to create issues which can complicate fertility or pregnancy.
Fibroid Symptoms
Fibroids are so common – and can be so small – that many women do not even know that they have them. Women with HLRCC often have moremore and much larger fibroids that are accompanied by other symptoms, including:
- Heavy bleeding
- A feeling of fullness in the pelvic area
- Enlargement of the abdomen
- Frequent urination
- Pain during sex
- Lower back pain
- Complications during pregnancy and labor
Diagnosis
Ways to find out if you have uterine fibroids:
- A gynecology (GYN) pelvic examination (a doctor can often detect larger fibroids just by feeling the abdomen).
- An ultrasound scan
- MRI scan
- Hysterosalpingogram – where dye is injected into the uterus
A pelvic ultrasound scan is usually performed transvaginally. However, when the uterus is very large, a transabdominal pelvic ultrasound may be needed to measure the full size of the fibroids and uterus. Some radiologists and gynecologists also perform a sonohysterogram in which a catheter is placed in the cervix into the uterus and fluid (sterile water or saline) is infused. Sonohysterograms can be helpful in determining whether there are fibroids within the uterine cavity.
Hysterosalpingogram is an x-ray test done during testing for infertility, and is used to investigate the shape of the uterine cavity and whether the fallopian tubes may be blocked. During hysterosalpingograms, radio-opaque material is injected into the uterine cavity and x-rays are done. Hysterosalpingograms can be helpful in determining whether there are fibroids within the uterine cavity or whether these fibroids compress the opening to the fallopian tubes. However they are not useful in looking at the fibroids themselves, and not all centers perform this procedure.
A gynecologist should continue these annual checks and consider adding radiological examination. Once a woman with HLRCC is known to have fibroids, a gynecologist should perform an annual examination to check for increasing uterine size suggestive of fibroid growth. Having imaging studies done over time (ultrasound or MRI) will also enable the radiologist and gynecologist to determine whether the fibroids have grown in size or number. Significant growth in fibroid size might suggest the development of a malignant type of fibroids called leiomyosarcoma. Thus, when fibroids grow rapidly, surgical treatment is usually recommended. Hysterosonograms and hysterosalpingograms may be helpful as a preoperative assessment for myomectomy (described below). While the first reports of HLRCC suggested that leiomyosarcoma might occur in women with fibroids, a large study at US-NIH has shown that fibroids may be atypical, but no cases of leiomyosarcoma have been observed.

From https://en.wikipedia.org/wiki/Uterine_fibroid
A moving story: “I was at the University of Michigan as a high-risk patient while I was pregnant with my first child,” said Julie Sherwood, a 39-year-old HLRCC patient. “I had a vertical c-section and they still could not find my baby because I had so many fibroids in the way. They had to do a second incision and the baby was saved. During my second pregnancy my fibroids tripled within weeks and the baby couldn’t survive. I had an emergency hysterectomy weeks later.”
Julie’s moving story, along with many other discussions about a variety of health-related topics, can be found in a radio interview at:
https://powerfulpatient.org/archive/2011/week1111_fibroids.php
Treatment
There are several options of managing fibroids. Many factors are considered to determine which option is the best one for each individual.
Sometimes a hysterectomy is recommended. During hysterectomy the uterus and cervix are removed, and sometimes the ovaries are removed as well. It is not possible to carry a pregnancy after the uterus is removed.
Another option for treating fibroids is a surgical procedure called myomectomy. During a myomectomy only the fibroids are removed, and thus the ability to carry a pregnancy may be preserved. When fibroids are within the uterine cavity, they may be removed through a hysteroscopic myomectomy procedure (operating using a viewing instrument through the cervix). When the fibroids are large and within the wall of the uterus, an abdominal myomectomy is usually performed. While some gynecologists perform this procedure laparoscopically or robotically (operating using a viewing instrument in the abdomen), it is important that the fibroids are not morcellated (mechanically cut up into pieces) inside your body. Removing the fibroid intact will enable the pathologist to examine it for atypical features or possible leiomyosarcoma. Additionally, there is a concern that many fibroids associated with HLRCC are atypical and cellular. With morcellation, small pieces of tissue left in your body may attach and grow. Another concern is the number of myomectomy procedures done prior to attempting pregnancy. If a woman undergoes several myomectomy procedures prior to attempting pregnancy, she may have difficulty becoming pregnant or may be at risk of miscarriage. These effects may occur because, for example, of scarring in the uterine wall. Thus, timing myomectomy surgery just before attempting pregnancy may be a preferable strategy.
Non-surgical treatments of uterine fibroids include Uterine Artery Embolization (UAE) or High Intensity Focused Ultrasound Ablation (HIFU) of fibroids. Both procedures are performed by an interventional radiologist. These physicians are trained in a medical sub-specialty of radiology which utilizes minimally-invasive image-guided procedures to treat diseases. At the present time, neither procedure is recommended for women with HLRCC as they will not investigate whether fibroids are atypical or cancerous. These strategies either lessen the flow of blood to the uterus (UAE) or physically destroy part of the fibroid (HIFU). In some patients with HLRCC who have undergone UAE, their fibroids have rapidly increased in size. A type of UAE called UFE (Uterine Fibroid Embolization) is essentially the same procedure as UAE (Uterine Artery Embolization). This article Complications of Uterine Fibroid Embolization 2006 by Brian E Schirf, Robert L Vogelzang, Howard B Chrisman has additional negative information *Expulsion or discharge of small tissue fragments and necrotic material is a common minor complication of UFE, occurring in 2.5% of patients from a study of 400 consecutive UFE patients.”. These small tissue fragments may relocate to other organs and start growing. Although benign this is similar to cancer metastasis.
Birth control pills and the levonorgestrel (MirenaTM) IUD decrease menstrual bleeding in women regardless of whether they have fibroids, and are effective methods of contraception. Women with the HLRCC gene defect are able to use these treatments for these indications. While fibroids do appear to be hormone-sensitive, it is unknown at this time whether using hormones like birth control pills or the levonorgestrel IUD will be effective in decreasing fibroid size in women with HLRCC.
There are many organizations and links that will assist in your understanding of uterine fibroids. Keep in mind that we are currently trying to educate these organizations about HLRCC and that you most likely will not find information specific to HLRCC on these websites.
The Center for Uterine Fibroids
https://www.fibroids.net
The National Uterine Fibroids Foundation
Colorado Springs, Colorado
(719)633-3454
https://www.huff.org
The following links provide additional information about fibroids:
- https://www.womenshealth.gov
- https://www.fibroidoptions.com/
- https://www.dbh.nhs.uk/Library/Patient_Information_Leaflets/WPR24900%20Hysterosalpingogra.pdf
- https://www.sirweb.org/patients/uterine-fibroids/
- https://www.revolutionhealth.com/conditions/reproductive-health/fibroids/index
There are additional links for fibroids to be found in the HLRCC Science document.
Renal (Kidney) Tumors
Note: This section of the Handbook is also relevant for some non-HLRCC tumors which are Fumarate Hydratase Deficient (FHdRCC).
Research indicates that only a proportion of individuals with HLRCC develop malignant (cancerous) kidney tumors. There is a higher proportion in the US-NIH study possibly because they are recruiting as kidney cancer specialists. The variation in incidence figures is considerable and may depend on several factors including methods of recruitment. It will take more studies to determine the true risk of kidney tumors in a particular individual. Meanwhile, since this is such a potentially lethal tumor, we recommend that everyone be screened for kidney tumors. See Suggested Screening Guidelines.
Diagnosis
Kidney cancer often develops with no initial symptoms, and by the time symptoms such as pain or blood in the urine appear, it has often already become a danger to life.
In the general population kidney cancer accounts for about 1-2% of all cancers. Renal Cell Carcinoma(RCC) is divided into groups : Clear cell, Papillary, Oncocytic and Chromophobe, Collecting Duct, Other Renal, Molecularly Defined. In Molecularly Defined there is Fumarate Hydratase-deficient renal cell carcinoma which includes RCC associated with HLRCC and also sporadic cases.
A person with a diagnosis of HLRCC has a much higher risk of developing lesions in the kidney compared to the general population. There are three kinds of lesions in the kidney: benign cysts, hard tumors, and hard lumps developing inside a cyst. Unlike other genetic syndromes associated with kidney cancer, HLRCC kidney tumors can metastasize (spread) when the tumor is relatively small (less than 1 cm). These tumors usually spread to the lungs, bone and brain. It was thought that HLRCC was generally unilateral in that only one kidney is initially affected. However as people are living longer after surgery, problems can develop in the remaining kidney. Like all kidney tumors they often initially have few, if any, noticeable symptoms, which is why scanning is essential in order to detect them at an earlier stage.
Although a kidney biopsy is now considered safe in the general population it should be avoided in HLRCC patients to avoid the possibility of spreading cancer cells. Instead, a diagnosis from MRI and CT scans is recommended by an HLRCC expert.
Treatment / Management of the Kidneys
This is an area which is still being actively researched and there are many factors to be considered for every individual. The key to managing HLRCC kidney tumors is surveillance to find tumors when they are small. Surgical removal if possible is currently the treatment of choice when a tumor is found. Some families report a currently healthy grandparent who had a nephrectomy many years ago, and there are people who had tumors removed 10 years ago who are healthy and well.
Once an HLRCC kidney tumor has metastasized, the prognosis changes, and the course of metastatic kidney cancer is similar to the experience of others in the general population. There are targeted molecular treatments that are currently in clinical trials. At the US-NIH there is a clinical trial of a combination of bevacizumab (Avastin) and erlotinib (Tarceva). In 2014 the initial report of the trial was very favorable. The spectrum of available drugs and the recommendations for primary and secondary therapies for papillary kidney cancer is evolving rapidly. Check with an oncologist experienced in kidney cancer and make contact with an HLRCC specialist with advice from info@hlrccinfo.org.
The type of kidney surgery is dependent on many factors. Sometimes it may be necessary to remove the entire kidney (nephrectomy) or a partial nephrectomy may be performed. A partial nephrectomy is nephron sparing surgery in which only the tumor and a little surrounding margin of tissue is removed. With HLRCC a wider margin should be used.
Follow-up after RCC
The exact follow-up procedure for every patient will vary from center to center and should be discussed and agreed with your physicians. We will only describe here examples of what you may expect.
If you have had a nephrectomy, then initially for the first 2 years a full chest and abdominal CT scan with contrast may be carried out every 6 months to check for any metastasis (spread). ALWAYS TELL THE RADIOLOGIST THAT YOU HAVE ONLY ONE KIDNEY AND PLEASE TO REDUCE THE AMOUNT OF CONTRAST.
A PET/CT and a bone scan may also be ordered if metastasis is thought likely. Kidney cancer will often metastasize to the lungs or bone. Note this is then called secondary kidney cancer in the lung or bone and NOT lung cancer or bone cancer.
After two years the screening interval may be increased to yearly, but there continues to be a life-time risk of either recurrence or metastasis requiring long-term surveillance. See https://www.ncbi.nlm.nih.gov/pubmed/21903243
Pheochromocytomas and Paragangliomas
Recently ~2013 it has been discovered that some pheochromocytomas and paragangliomas are related to Fumarase Hydratase (FH) Gene – HLRCC .
By kind permission from the VHL Alliance, this comprehensive section is copied from its Handbook. Although the section is with reference to VHL it can be regarded as also relevant to HLRCC. Most HLRCC diagnosed people will never develop a pheochromocytomas (PCC) or a paraganglioma (PGL) in their lifetimes but the possibility exists and patients and physicians should be aware of their symptoms.
 The adrenal glands are glands in the body that are approximately 3 x 2 x 2 cm (1 in long) and sit on top of each of the kidneys (see Figure 9). They produce hormones that are involved in the regulation of critical body functions, including:
The adrenal glands are glands in the body that are approximately 3 x 2 x 2 cm (1 in long) and sit on top of each of the kidneys (see Figure 9). They produce hormones that are involved in the regulation of critical body functions, including: - Catecholamines: This is predominantly epinephrine, but also some norepinephrine. Epinephrine helps to regulate the “fight or flight” response to stress (also known as adrenaline. It is the main catecholamine produced by the adrenal glands).
- Glucocorticoids: The most important glucocorticoid is cortisol. Cortisol helps to regulate blood sugar, blood pressure, fat and protein metabolism, and the immune system. Cortisol is known as the ‘stress hormone.’
- Mineralocorticoids: The most important mineralocorticoid is aldosterone. Aldosterone works mainly in the kidneys by maintaining salt and water balance within the body. This is important for blood pressure regulation and proper cardiovascular function.
- Adrenal androgens: These are precursors to sex hormones (i.e. testosterone, estrogen).
Go to the Top
Pheochromocytomas and Paragangliomas
VHL is associated with a usually benign type of tumor occurring in the adrenal glands, called a pheochromocytoma (pheo). Pheos occur more frequently in some families than others. They are rarely malignant (less than 7% of the time) among people with VHL. Detected early, pheos do not cause problems, but they are potentially lethal if not treated. This is especially true during times of heightened stress (surgery, accidents, childbirth, etc.).
Pheos that develop outside of the adrenal glands are called paragangliomas (paras) and are very rare, even in VHL patients. Paragangliomas may occur anywhere on the sympathetic nervous system, which includes anywhere along a
line drawn from the groin to the ear lobe, on either side of the body. Multiple tests may be needed to find them.
Research indicates that adrenal tumors are as much as four times more common among people with VHL than previously thought. Even in families that have not previously had a pheo, it is still important to test for the presence of these tumors. In one large progeny in France where there were no pheos for three generations; there are now pheos in two branches of that family.
Go to the Top
Symptoms
The primary clinical sign of a pheo is high blood pressure, especially spiking blood pressure, that can put strain on the heart and vascular system, potentially causing a heart attack or stroke. However, blood pressube normal, despite the presence of a pheo. Patients may notice headaches, irregular or rapid heartbeat, or what feels like a panic attack, fear, anxiety, or even rage. There may be unexplained heavy sweating and sometimes people experience hot and/or cold flashes. There may also be abdominal pain or unexplained weight loss. It is recommended that all people with VHL be screened regularly for pheos.
Go to the Top
Testing for a Pheochromocytoma
It is extremely important to test for pheochromocytomas before undergoing surgery for any reason, as well as before going through childbirth. Undergoing either of these stressful experiences with an undiagnosed pheo can be extremely dangerous. If the doctors are aware that the pheo is there, they can take preventive action that will ensure the safety of the patient and of any unborn child.
Traditional blood or urine tests that measure only catecholamines are inadequate to find most pheos. In order to diagnose a pheo, an initial biochemical test is done to measure blood or urine metanephrines. The preferred test is a
plasma free metanephrines test, due to its higher sensitivity. This involves taking a sample of blood and measuring the levels of metanephrine, the metabolite of adrenaline, and normetanephrine, the metabolite of noradrenaline. More widely available is the fractionated 24–hour urinary free metanephrines test, which includes collecting a 24–hour urine sample and analyzing it for fractionated metanephrines and normetanephrine.
The measurement of normetanephrine is most important, since VHL–related pheos usually do not produce adrenaline or its metabolite, metanephrine, in significant amounts. Testing for methoxytyramine (a metabolite of dopamine) levels may be useful in evaluating metastatic status, although only 17% of VHL patients with pheos produce it. If additional information is required, or if there are symptoms of a pheo, but the blood and urine tests are negative, anatomical imaging scans should be used.
Go to the Top
Testing Standards for Pheochromocytomas and Paragangliomas
Below are the clinical guidelines that were approved by the Endocrine Society for testing for the presence of pheochromocytomas and paragangliomas (together known as PPGLs):
- Surveillance for PPGLs should always include measurements of plasma metanephrines (obtained from a blood sample) or urinary fractionated metanephrines (obtained from a urine sample).
- For a blood sample, it is recommended that patients be supine (lying down) for a minimum of 20–30 minutes between the time the needle is inserted and the time the blood is drawn. Studies have shown that seated blood testing more often results in false positives. The reason for this is that the release of catecholamines by peripheral nerves and the adrenal gland is stimulated by an upright posture. Sitting upright results in increased blood levels of metanephrines compared to being in a supine position.
For blood sample analysis, upper reference intervals (the test result above which a pheo is determined to be present) should be established from supine tests, not seated tests, in order to minimize the chance of a false negative result (missing a PPGL that is present).
Analysis is performed using liquid chromatography (LC–MS/MS) with mass spectrometric, or electrochemical detection and using supine norms for plasma test results. All positive test results should be followed up. Follow–up may involve repeated biochemical studies (e.g. a clonidine test), or a CT scan or MRI (if a CT scan is not appropriate).
In VHL, it is only necessary to consider elevations of normetanephrine. For plasma in an adult patient with VHL, anything over 112 picograms/milliliter (0.61 nanomoles/liter, the NIH upper reference limit) should evoke suspicion. Anything over 400 pg/mL (2.2 nmol/L) for a sample that is taken with the patient lying down
and relaxed (no stress) and on no antidepressants is immediately highly suspicious (close to 100% likelihood). Imaging is then warranted. Between those ranges, the likelihood of a pheo increases with increased level and follow–up tests, such as imaging, should be considered.
If these chemical tests indicate the presence of a pheo, but it cannot easily be located on MRI or CT, an MIBG or PET scan may be recommended. These scans help to locate a pheo, even if it is outside the adrenal glands.
According to research at the U.S. National Institutes of Health, different tests
have different success rates in locating a pheochromocytoma or paraganglioma:
- 18F–FDA PET scan finds 75–92%
- 18F–FDOPA PET scan finds 67–93%
- 123I–MIBG scan finds 67–86%
- 18F–FDG PET scan finds 83–93% (adrenal: 67%)
- Octreotide scan finds fewer than 50% of these tumors. Please note that the Octreotide scan will soon be replaced by 68Ga–DOTA analogs used with PET scans.
The choice of one of these tests is often made depending on the availability of a particular technology at that center. However, it is important to note that if the test chosen does not find the pheo, there is still some chance that the pheo is there but cannot be detected by that particular test. A second opinion should be requested from a VHL or pheochromocytoma expert.
Go to the Top
Preparing for Pheochromocytoma Testing
The accuracy of the urine and blood tests for pheo activity will be determined in large part by your own cooperation in preparing for the test. The tests are most reliable when care is taken in two areas—diet prior to testing and preservation of the urine sample from the start of the test until the lab processing is complete.
For a reliable measurement of plasma and urinary free metanephrines, no specific diet is required. Testing for plasma or urinary 3–methoxytyramine requires a diet poor in catecholamines to prevent false–positive results. Catecholamines can be found in fruits (such as bananas), fruit drinks, and nuts.
While there is no strong data that suggests that regular use of tobacco or alcohol may be linked to inaccurate results, caffeine should be avoided because it can cause false–positives on some tests. Certain drugs and medications can interfere with the measurement method being used, while others, like antidepressants, can cause false–positives. Be sure to tell your doctor and the technician if you are taking any medications. If possible, testing for pheos should be done before beginning any medications.
Specific instructions may differ slightly from center to center, due to different methods of analysis. Follow any instructions carefully to avoid a false reading.
Go to the Top
Preparation for Blood Testing
The procedure usually takes about 45 minutes. It is important that you be quiet and calm for 20–30 minutes prior to the blood draw to ensure accurate results. Bring something with you to keep you occupied and relaxed as you will be
asked to lie quietly on a table for 20 minutes after the needle is inserted before
the test begins.
| UPPER LIMITS | ||
| Normetanephrines | Metanephrines | |
| Boys (ages 5–18 years) | 97 pg/mL (0.53 nmol/L) | 102 pg/mL (0.52 nmol/L) |
| Girls (ages 5–18 years) | 77 pg/mL (0.42 nmol/L) | 68 pg/mL (0.37 nmol/L) |
Table 4. Published upper limits for reference intervals of plasma concentrations of metanephrines in children (from samples collected lying down with an indwelling i.v.).
Reference intervals for each lab may be slightly different due to variations in processing.
If there are concerns about interactions with medications, it is important that the laboratory use LC–MS/MS techniques to analyze the sample, in order to achieve the highest sensitivity and selectivity in checking fractionated
metanephrines, especially normetanephrine.
Go to the Top
Preparation for 24–hour Urine Testing
Pro Tip: Do not begin collection on Friday or Saturday. This ensures that your sample will be delivered to the lab on a working day and can be processed promptly.
1. Start the collection in the morning. Empty the bladder; do not save this urine specimen.
2. Write the date and time on the jug. (If there is a preservative added to the jug, be careful not to get it on the skin. If this happens, wash the area immediately with water.)
3. Save all the urine passed for the next 24 hours in the jug provided including the final specimen passed exactly 24 hours after beginning the collection.
4. Keep the urine refrigerated at all times. You might keep it in a paper bag in the refrigerator. If you must be out, you could carry it in a bag or backpack with plastic ice packs against the jug.
5. Write this date and time on the jug when the collection is finished.
6. Bring the collection and the paperwork to the lab as soon as possible after collection. (Labs are usually open early in the morning or have a place where you can arrange to drop it off early.)
Go to the Top
Treatment
If surgery is required, the preferred method is a cortical–sparing partial adrenalectomy. Studies have shown that keeping even a small amount of the cortex of the adrenal gland, if surgery on both glands is required, makes it easier to manage post–surgery. It also usually avoids the need for steroid replacement.
On the other hand, it must also be recognized that the remaining adrenal tissue can be associated with recurring pheos. Removal of the entire adrenal gland is rarely required to manage VHL–associated pheos.
The “key hole” operating technique (laparoscopy) is currently used to treat pheos. With this technique, there is less risk of infection and the recovery is much faster. Some surgeons have the technology to simultaneously remove pheos located on each of the two adrenal glands. Laparoscopic or robotic surgery should be discussed with your doctor.
Prior to surgery, the medical team will prescribe “blockers” (alpha blockers, sometimes followed by beta blockers), or drugs that inhibit the formation of catecholamines. These medications will calm the effects of the chemicals produced by the pheo and allow the surgery to proceed calmly, without causing a pheo crisis. While the blockers will make you tired, they are critically important.
They may be prescribed for two or more weeks before the planned surgery.
Another important consideration before surgery is to make sure that the anesthesiologist working with your surgeon has experience with pheos. The anesthesiologist is responsible for managing your blood pressure during the surgery. Your endocrine surgeon should be able to let you know who will be part of your surgical team.
Go to the Top
Adrenal Dietary and Lifestyle Management Strategies
Maintain a healthy diet. Chronic stress is associated with increased levels of cortisol, a hormone related to stress which helps regulate blood sugar, blood pressure, fat and protein metabolism, and the immune system. High levels of cortisol can promote overeating and lead to weight gain. Eating a balanced and nutritious diet supplies the body with all its essential nutrients and can be useful for controlling weight, reducing stress, and improving performance.
A clinical study evaluating the effect of calorie restriction for one month in
otherwise healthy overweight women aged 20–36 found that, along with an
average weight loss of almost 13 pounds, there was a significant decrease in blood
pressure, heart rate, and cortisol hormone levels, improved hand–eye
coordination, and no evidence of increased physiological or psychological stress.
Work with a dietician to develop the most appropriate diet for you.
Eat salt and stay hydrated. Those who have had their adrenal glands removed due to pheochromocytomas or who have adrenal insufficiency (or Addison’s Disease) generally need more salt in their diet. This is because they do not have enough of a hormone called aldosterone, which regulates sodium and potassium (salt and electrolyte) levels in the body. Aldosterone is produced by the adrenal glands, and without functioning adrenal glands, there is very little or no aldosterone production. If aldosterone levels get too low, the body loses too much sodium.
People who produce low or no amount of aldosterone are often categorized as “salt–wasters” because they cannot maintain salt (sodium) levels. These individuals must take supplements to replace aldosterone. Even with replacement, maintaining optimal levels of aldosterone can be a challenge. When these “salt wasters” exert themselves heavily or spend enough time in hot temperatures, there is a good possibility of their losing too much salt in sweat and urine, putting them at a higher than normal risk for dehydration. Therefore, “salt wasters” should be sure to drink enough non–sugar–loaded liquids and supplement with enough salt to alleviate this dangerous situation. Good liquid options include water (always the best choice), seltzer or soda water, tea of any type, fruit juice, milk, broth, etc.
Avoid simple carbohydrates. Cortisol is released by the adrenal glands if the body has low blood sugar. Low levels of glucose can occur when meals are skipped or taken at irregular intervals. Eating simple or refined carbohydrates (such as sugar, corn or table syrup, or white flour) can also cause low blood sugar levels, since they are digested and absorbed very quickly by the body. Instead of a gradual rise in blood sugar, this quick absorption triggers a quick spike in blood sugar levels that is followed by a quick decline. This rapid increase and decrease in blood sugar levels causes an increase in cortisol levels, which triggers the stress response mechanism.
Eating meals at regular intervals and consuming foods other than simple carbohydrates can prevent this increase in cortisol levels. Proper diet is important not only to control blood sugar and reduce spikes in stress hormone levels, but also to reduce risk factors for disease.
Limit stimulants. Consumption of stimulants, such as energy drinks, coffee,
or soft drinks has been linked to feeling stressed. The effect of caffeine is known to increase cortisol hormone production and intensify the stress response.
Therefore, caffeine should be consumed in moderation or avoided by people exposed to chronic stress or with impaired adrenal function. Smoking cigarettes can also increase stress; nicotine exposure is known to increase cortisol levels.
Stay positive, practice self–care. Low self–esteem and loneliness are known to increase cortisol levels, while maintaining a positive outlook on life and a good social support system is associated with lower stress hormone levels.
Sleep. There is a known association between sleep and levels of cortisol, the stress hormone. While getting enough quality restful sleep can slightly decrease cortisol levels, disturbed sleep or not getting enough sleep can lead to mildly increased cortisol levels. For this reason, sleep deprivation may be an important risk factor leading to stress–related disorders.
Medication. Please note that if you have had both of your adrenal glands completely removed, it is important to follow your prescribed daily doses of hydrocortisone and fludrocortisone, and to be checked regularly by your endocrinologist. These medications work to replace the functions of your missing adrenal glands to manage the balance of fluids in your body, maintain kidney function, control blood pressure, and maintain cardiovascular health.
TYPES OF SCANS
There are four types of Kidney Imaging: Magnetic Resonance Imaging (MRI), Computed Tomography (CT), Positron Emission Tomography (PET) and Ultrasound. Some centers will alternate MRI with CT scans. The kidney cancer of HLRCC can metastasize (spread to other organs or bone) even when small, which makes early detection essential. There are several well-used methods to visualize kidney tumors. There are pros and cons for each.
Magnetic Resonance Imaging (MRI)
MRI scans with and without contrast is an acceptable method to examine kidneys. This process creates images using magnetic waves. No radiation is used.
The MRI scan for HLRCC patients should use pre-and post-contrast 3D acquisition with as high a resolution as possible, 3mm or less slice reconstruction is advised. Clinicians at the National Institutes of Health are currently using 1mm slice reconstruction in this population. The scans should be reviewed by someone with expert HLRCC knowledge especially if kidneys cysts are present. The preferred option is to use MRI with gadolinium contrast, because it is the contrast medium that identifies soft tissue. Please make sure that specific contrast agents are used (macrocyclic agents, not linear agents). Gadobutrol is one example. See Extracellular Gd agents . There is some concern that repeated use of gadolinium contrast may build up in the body tissue and some people have serious side effects from the contrast agent. It may be possible to get sufficient quality images without using gadolinium contrast. MRI scanners have recently improved with “Open MRI” and shorter and wider tunnels making the experience less problematic even for people with mild claustrophobia. However, there is some concern that the image quality may be reduced with some open large bore MRI scanners. The objective is to get the best possible picture quality. If you feel you need calming medication for anxiety or discomfort, a larger bore to accommodate larger body mass, or any other requests, negotiate a solution that will give the doctor the picture quality needed while addressing your concerns. Ask: Is it possible to enter the MRI machine feet first? People find this is an improvement on the unpleasant experience. Note: Breast tissue expanders with magnetic ports are MRI unsafe, preventing patients from benefiting from the diagnostic capabilities of MRI.
Computed Tomography (CT Scan)
CT scans with and without contrast is an acceptable method of visualizing kidneys. However, images are created through the use of radiation. Annual CT scans over a life span raises concerns about using up your lifetime maximum of radiation exposure.
The CT scan is done with a contrast agent usually containing iodine and you should drink plenty of water afterwards to flush the contrast agent out of your body. If there is any doubt about your kidney function (creatinine levels above 1.6) you may be given 500cc of saline solution first and Visipaque(iodixanol) or Omnipaque (iohexol) contrast which have lower iodine content. The unpleasant, oral, barium-based contrast used to distinguish the digestive organs has been phased out in the U.K. and replaced with just drinking plain water. Radiologists in the U.K. said it was just as good.
Computed Tomography Photon-Counting
This photon-counting CT Scan is using new technology (2021) at NCI/NIH to give improved scans with less radiation see pubs.rsna.org/doi/10.1148/radiol.2018172656 for a description of it.
Positron Emission Tomography (PET)
For ordinary RCC, PET scans are normally less effective than CT scans with contrast and have been known to give false negatives. A PET scan is often combined with a CT scan. However, with HLRCC any tumors present are glucose hungry and PET can be a useful diagnostic tool especially for detecting metastases. There can be false positives in both the adrenal glands and the uterus because of the presence of benign HLRCC related tissue. Cancer cells upregulate glucose metabolism, which is a phenomenon known as the Warburg effect. This is the basis for PET in which a glucose analog tracer FDG (2-18fluoro-2-deoxy-D-glucose), a radioactive modified hexokinase substrate, is used to differentiate between normal and tumor tissue.
You may be offered a “delayed PET scan” see Advantage of delayed whole-body FDG-PET imaging for tumour detection.
Ultrasound
Ultrasound can be effective in visualizing some kidney tumors, but can easily miss the small tumors associated with HLRCC or does not detect some types of tumor tissue. Ultrasound is used occasionally when a tumor is present to determine the amount of fluid in the mass. Note: Ultrasound as a screening (surveillance) method is not recommended for people with HLRCC.
Bone Scan
A bone scan consists of taking a camera image of your body about 3 to 4 hours after giving you an injection of a radioactive isotope. This can detect any metastasis that has spread to the bones.
Scan Contrast Agents Recommendations
Keep well hydrated before and after your scans as the contrast agents are excreted through the kidneys. It will also help your veins to be found. Some centres recommend no food or drink for 4-6 hours prior to MRI abdominal scan. However with no food, water is absorbed into the blood stream in as little time as 5 minutes.
Current research indicates that the gadolinium contrast used in MRIs DOES NOT harm the kidneys and can be used in all patients except those on dialysis or are pregnant. CT scans are also good and are sometimes used in place of MRI. When used judiciously, the amount of radiation exposure due to CT scans is not problematic in adults. MRIs cannot be used in those with pacemakers or magnetic metallic material, or in cases of claustrophobia when anesthesia may be needed. Please make sure that specific contrast agents are used (macrocyclic agents, not linear agents). Gadobutrol is one example.
People with reduced kidney function, as indicated by low creatinine clearance, need to be protected from any side effects of the iodine contrast dyes used for CT scan. The principal goal is to ensure that the patient has sufficient fluid in the body to flush the contrast dye out in a timely manner. Generally, iodine contrast for CT scans can be given to those with an estimated GFR (glomerular filtration rate) of 40 or higher. Radiology teams may take certain safety steps, such as extra flushing or safer versions of contrast, depending on their hospital protocols.
For patients who are already on dialysis, it is generally safe to obtain a CT scan with iodine contrast, but they must have dialysis within 24 hours afterwards to avoid complications. The alternative is an MRI without contrast with T1, T2, and fat suppression sequences, which can help partially make up for the lack of contrast.
Criteria for gadolinium used based on Glomerular filtration rate (GFR):
• Patients with an estimated GFR of less than 60 and greater than 30, hydration with 1 liter of bicarbonate solution infused over the course of one hour immediately prior to when IV contrast injection is performed.
• For those on long-term surveillance and estimated GFR over 60, a full dose of gadolinium is used, for estimated GFR of 30–60, ½ dose, and no contrast agent is used if estimated GFR is less than 30.
• People with renal failure (estimated GFR less than 30) can be followed without use of contrast agents using non-contrast MRIs with T1, T2, and fat suppression sequences, which can help partially make up for the lack of contrast.
SUGGESTED SCREENING GUIDELINES
There is now a published guideline by the world’s experts which corresponds generally to the information presented in this HLRCC Handbook.
2024: Note the Age of 8 in the sections below was chosen because the youngest HLRCC child with RCC was 9 years old. NIH now report a child of 7 years old so maybe an earlier screening age is now required.
Hereditary leiomyomatosis and renal cell cancer (HLRCC): renal cancer risk, surveillance and treatment. Menko FH, Maher ER, Schmidt LS, Middelton LA, Aittomäki K, Tomlinson I, Richard S, Linehan WM, 2014
A paper describing that screening at various starting ages compared with not starting is cost-effective at every starting age considered Cost-effectiveness model of renal cell carcinoma (RCC) surveillance in hereditary leiomyomatosis and renal cell carcinoma (HLRCC) Alexander J Thompson, Yousef M Alwan, Vijay A C Ramani, D Gareth Evans, Eamonn R Maher, Emma R Woodward, 2022
Before following these guidelines please read the section on obtaining life insurance as it may be more difficult to obtain afterwards.
If you are having difficulty with testing from your center please contact a VHL Alliance Clinical Care Center for advice and support. These centers are used to screening VHL patients from birth and HLRCC is a VHLA project. Please feedback to HLRCC Foundation should there be any problems making this approach.
https://www.vhl.org/patients/clinical-care/ccc/
This will lead you to a directory with tabs for US and International.
HLRCC Foundation Suggestions From Birth
The HLRCC Foundation has taken a stronger position based on input from its members.
1) As informed patients or as parents we should be able to strongly suggest FH genetic testing from any age starting from birth. This is justified from the fact that new research has shown that some pheochromocytoma and paraganglioma are associated with FH and can manifest from birth. This also means that children under the age of 16 can either be warned that they have HLRCC FH mutation or are clear and don’t need to worry because they don’t have it. Many children become worried about not knowing and are able to cope well with a positive diagnosis.
2) As informed patients or as parents we should be able to strongly suggest that screening with an initial MRI test can start from any age from birth for anyone at risk. For a child of a HLRCC patient the child is at risk either known from a genetic test or because of parenthood if no genetic test has been made, or if no family FH mutation is known which occurs in a few families. To screen every year with MRI may be considered excessive if the initial MRI is clear and maybe 2 or 3 year intervals is more appropriate with ultrasound in between. This of course slightly increases the risk of something developing and being undetected for a period of time.
—————————————
The one common guideline we do recommend is that you take charge. Be informed, discuss openly with your medical professionals and consider the pros and cons. Please e-mail us at info@hlrccinfo.org if you want more information about the published guideline above or you have unanswered questions and we will always try to help you.
HLRCC is a relatively young condition in that there are few people who have been followed medically from childhood through adulthood with today’s screening technologies. We have lots of questions, but few firm answers at this time. However everyone with HLRCC can assist us in learning what we need to know to protect ourselves and our children from the worst effects of HLRCC.
The purpose of screening guidelines is to help patients and their local physicians watch out for foreshadowing of problems, before they get to a critical stage. By intervening at earlier stages, hopefully these problems never become threatening to life or quality of life. Note that screeningmeans that you do not yet have any issues in the area being screened. Once you have a diagnosed issue, then you will need to follow the guidance of your health care team in deciding what course of action to take. Feel free to seek a second opinion from a doctor more familiar with HLRCC, even in another country. Scans can easily be sent through the mail, and the experts are quite willing to provide their opinion. Note: e-mailing scans is not satisfactory. There are many file formats used by the various vendors, so the receiving doctor will likely not be able to read the file. On the CD they include the viewer software to read the file, so the receiving doctor can open the file and read it quite nicely. Sending a universal format (like a .pdf) reduces the quality of the image, making it hard to determine what is a cyst and what is a tumor – a critical distinction for us.
- MRI is recommended in order to minimize exposure to radiation. There is some concern that repeated use of gadolinium contrast may build-up in the body tissue and some people have serious side-effects from the contrast agent. It may be possible to get sufficient quality images without using gadolinium contrast.
- CT should be reserved for times when they are needed to answer some specific diagnostic question or in planning surgery.
- Ultrasound of the kidney is not recommended, as ultrasound is very much dependent upon the quality of the machine and the skill of the operator. Ultrasound is better than nothing, but is unlikely to find tumors less than 1 cm, leaving a wide opportunity for risk in HLRCC.
The screening guidelines shown in this section are the best advice we were able to assemble at this time from the major research teams studying this condition, and from patient experience. We are hopeful that using these guidelines as a starting point, and with feedback from patients and physicians worldwide, we can evolve these guidelines over the next several years to make them increasingly cost-effective.
Upon HLRCC Diagnosis (At Any Age Greater Than 8)
- Annual full-body skin check by a dermatologist to note the location, number, and stage of skin bumps
- For all, annual MRI of the abdomen, looking for kidney tumors, noting number and size of any cysts or tumors seen. The MRI scan for HLRCC patients should use pre-and post- contrast 3D acquisition with as high a resolution as possible, 3mm or less slice reconstruction is advised. Clinicians at the National Institutes of Health are currently using 1mm slice reconstruction in this population. The scans should be reviewed by someone with expert HLRCC knowledge especially if kidneys cysts are present.
- Adults may be offered a CT scan as well as an MRI for their first appointment in order to have a baseline scan for comparison with any later scans
- For women starting at the age of 21, annual examinations by a gynecologist to enable screening for fibroids. You should inform the gynecologist that you have the HLRCC condition, of any family history of fibroids and stress the importance of looking for even small fibroids.
For Children at Risk Under 8
Children are “at risk” if they are not genetically tested or if they are in the 3% of families which have clear evidence of HLRCC symptoms, but no DNA alteration can be found.
Annually from age 1
- Full body skin check by the pediatrician, noting any skin bumps. If present, refer to a dermatologist familiar with HLRCC
Annually beginning at age 8
- Full-body skin check by the pediatrician noting any skin bumps. If present, refer to a dermatologist familiar with HLRCC
- MRI scan of the abdomen to check for any cysts or tumors of the kidneys. The MRI scan for HLRCC patients should use pre-and post- contrast 3D acquisition with as high a resolution as possible, 3mm or less slice reconstruction is advised. Clinicians at the National Institutes of Health are currently using 1mm slice reconstruction in this population. The scans should be reviewed by someone with expert HLRCC knowledge especially if kidneys cysts are present.
Feedback – You Can Help Us Learn
Each time you do your annual check for any family member, would you please keep a log of the results? It is just as important for us to know that “all is well” as it is to hear that something was found. There is now a is a patient registry for HLRCC, FD, VHL, BHD, and SDHB patients for entering your HLRCC medical information. Please register with MyVHL: Patient Natural History Study (Previously CGIP Databank- Cancer in Our Genes International Patient Databank) hlrccinfo.org/myvhl-cgip-databank
Meanwhile, if you could please keep a paper notebook of this information, you will be able to add it when the online service is available. You will have an account and password to enter your information. Our goal is to analyze the medical information (without your personally identifying information) to determine at what ages the various issues are likely to emerge, and whether earlier intervention might be helpful. For example, there are new treatments for fibroids that might be used on smaller fibroids so that they never advance to the stage where hysterectomy is the only remaining option. See the fibroid section for treatment recommendations.
- Date
- Name of patient
- Date of birth
- Age of patient
- Skin check – please note what if anything was found. Include the location of any skin bumps, their color, number, and stage of development.
- Fibroid check (females only)
- Kidney check – note any cysts or tumors found. This information will be spelled out in the written report from the scan. It would be a good idea for you to obtain a copy of this report and keep it in your notebook so you have it to refer back to in future.
- Check for pheochromocytomas and paragangliomas as some have been found to be associated with HLRCC.
- Any other health issues, whether or not they seem to be connected to HLRCC. Include blood pressure reading, any symptoms of kidney stones or infections, any irregularities in periods for females, any abnormalities noted in male scrotal exams, prostate, or epididymal cysts.
- Any treatments recommended?
COMMONLY ASKED QUESTIONS
Who has HLRCC?
Males and females from birth, but most symptoms occur after puberty, which may begin as early as 8-9 years of age.
Should I get tested?
If one of your parents is positive for HLRCC, it is very important that you obtain a genetic test for yourself, either through the study at the US-NIH or through a genetic counselor. Remember – there is a 50% chance that you are negative. You will not be able to advocate for yourself and your family until you know for certain if you have HLRCC.
What is FH and why is it important to HLRCC?
FH stands for Fumarate Hydratase, an enzyme associated with the Krebs Cycle that naturally suppresses tumors. Individuals with HLRCC have a lower FH level than those without HLRCC.
Is there anything I can do about an FH enzyme deficiency?
At this point there is no enzyme replacement for FH, but refer to our HLRCC Science document for the current research on enzyme replacement.
If I have HLRCC and have a child, should I have him/her tested?
This is a complex issue and there is no single answer or recommendation. We have written in this handbook a complete section on testing and screening as it is such an important issue.
What do I tell a child?
The level of information must be chosen to correspond to the child’s age and their ability to understand. A genetic counselor is trained to help you in this and often is involved in an interview with the child. Obviously you don’t want to scare the child, but hiding the simple facts by not discussing them may cause problems, especially with older children who can find out information by themselves and be more alarmed than is necessary. Children often have a surprising ability to cope with difficult news. Older children may be very angry with their parents if they feel that information was withheld from them when they were younger.
Is HLRCC a cancer?
Despite its name the majority of people with HLRCC never get kidney cancer and many people will go through life never knowing that they have HLRCC. Most of the tumors associated with HLRCC are not cancerous. The cutaneous leiomyoma (skin bumps) and uterine fibroids are problematic but benign. Some people (a minority) develop kidney cancer; but knowing about a genetic alteration and being able to screen for a cancer is a gift – an early warning system that most people do not have. It is best to find and treat kidney cancer before it has spread (called metastasis).
I am scared, how can I support myself and my family emotionally?
You have come to the right place. The HLRCC Foundation, found on the https://www.hlrccinfo.org site, has the information that you need. We also offer an e-mail address to send your questions to, a telephone number to discuss your concerns, and an online discussion at INSPIRE and RareConnect HLRCC Community in conjunction with other hereditary kidney cancers. We hope that you’ll use these resources!
Further Reading – Internet Sites
Please refer to our HLRCC Science document for an extensive list of research articles. If you find an interesting article, please feel free to e-mail it to us as well!
YOUR EMOTIONAL HEALTH
HLRCC can be an overwhelming diagnosis because of the word cancer. Although most HLRCC patients never get kidney cancer, dealing with the potential of developing it can be difficult. Others on this site may have learned of their HLRCC diagnosis AFTER developing kidney cancer and are currently undergoing medical treatment. No matter what stage you are experiencing, it is important to find emotional support to get you through this difficult time.
Some normal feelings after a diagnosis:
- Shock and Denial
- Fear and Worry
- Anger
- Sadness
- Acceptance and Coping
It can take one to two years after a diagnosis for life to return back to normal… and “normal” still means annual screening and always knowing that kidney cancer is a possibility. Having our children and family members tested can add to the stress of this diagnosis as well.
Being able to cope emotionally is essential for staying healthy and fighting cancer. Stress is very powerful and too much stress can hurt the body’s immune system. There are many things that you can do to help combat stress:
- Find time to exercise.
- Eat well and avoid tobacco, limit alcohol to 1-2 glasses per day and limit caffeine excesses.
- Get a good amount of sleep.
- Surround yourself with positive people and family members/friends who will offer you emotional support
- Find a support group to talk with about your feelings and fears.
- Attend individual, couple or family counseling.
- Become educated about HLRCC so you feel in control of your diagnosis. Purchase or download our handbook for detailed information.
- Find time to recharge your batteries. Depending on the type of person you are either “Find quiet and alone time to clear your head” or “Find time to be with other people”.
- Manage your stress, so that you feel more in control of your life. Use meditation, prayer, sports, walking, classical music, a bubble bath… to add something into your life that soothes you and helps you manage your stress level.
- Stay positive
The HLRCC Foundation is a wonderful support group of people and they can be found via the website hlrccinfo.org, in our HLRCC Community on Smart Patients on Inspire, and on Rare Connect as well. We also have an active Private Facebook Group. If you need a place to ask questions, find emotional support and talk about your own fears and feelings, please join us. See next section “PATIENT and MEDICAL SUPPORT”
PATIENT and MEDICAL SUPPORT
HLRCC Foundation Website
https://www.hlrccinfo.org
This is the home page for the HLRCC Foundation web site and provides the central contact point.
Smart Patients
We strongly advise that you join the HLRCC Community in Smart Patients.
Hereditary Leiomyomatosis and Renal Cell Cancer
community at
https://www.smartpatients.com/communities/hlrcc
If you are affected by kidney cancer also join the Kidney Cancer Community in Smart Patients.
https://www.smartpatients.com/communities/kidney-cancer
Public launch April 2013 – This is a new, free state-of-the art website. Smart Patients has many online communities serving medical conditions for patients and caregivers. The site includes a clinical trial search engine that presents trial data from ClinicalTrials.gov in a patient-friendly format as well as a general search engine for all the site.
It replaces the patient-to-patient message board support KIDNEY-ONC and PAPILLARY-RCC from the Association of Cancer Online Resources (ACOR).
Facebook Private Group
It is important that you understand that membership of this Facebook Group is controlled by administrators in order to protect your privacy. “Private” means that all posts within the group can only be seen by group members, and names of all of its members are not externally visible. There is no internal visibility to search engines and nothing on your Facebook Timeline.
Unless you are an existing family member, admittance requires you to submit relevant strictly confidential information about your reasons for wishing to join the group.
This can be done by emailing admin@hlrccinfo.org from the email account that is connected to your Facebook account.
If your request is acceptable you will receive an email from Facebook with a Facebook link inviting you to join the group. Using this link will enable your admission to the group to be finalized.
We strongly advise you to join and make friends. Members are finding this is a very easy way to communicate with each other. However it has inferior history search facilities compared to Smart Patients.
RareConnect HLRCC Community
RareConnect HLRCC Community
This is a new support community for HLRCC in the organization RareConnect a partnership of Eurordis and NORD “Connecting Rare Disease Patients Globally”. It is an alternative to INSPIRE, but has the advantage of providing language translation facilities. You can look in on RareConnect and then decide if you would like to join by creating your own user name and password.
INSPIRE
https://vhl.inspire.com
The VHL Alliance Group in INSPIRE supports HLRCC and BHD as discussion topics. It provides private patient to patient message board support. It allows patients to talk with each other about their questions and concerns, while providing emotional support to one another. You can also write your own journal entries or start or add to discussion threads. There is privacy control. We strongly advise you to join and make friends.
You can look in on INSPIRE and then decide if you would like join by creating your own user name and password. New topics are posted every day (there are many other topics discussed other than the specific medical issues of HLRCC) and it’s a very easy way to connect with others who are impacted by HLRCC and related hereditary kidney cancer syndromes.
VHL UK/Ireland Charity
VHL UK/Ireland Home Page This is a charity for UK/Ireland created to support families and carers for the allied genetic conditions of VHL, BHD and HLRCC and to raise money for research. The website gives contact information by telephone and into the private Facebook group.
Kidney Cancer Forums
These provide forums and message boards for Kidney Cancer.
![]() UK Action Kidney Cancer https://www.facebook.com/groups/195838270483807/
UK Action Kidney Cancer https://www.facebook.com/groups/195838270483807/
Connected to the forum site actionkidneycancer.org/
Action Kidney Cancer (previously KCSN – Kidney Cancer Support Network now merged with Renal Cancer Research Fund) is a patient managed national charity working directly with patients, carers and healthcare professionals to provide everyone touched by kidney cancer with the best possible support, information and advocacy.
https://www.kidneycancer.me/ This is connected to the Kidney Cancer Association see https://www.kidneycancer.org/
https://www.topix.com/forum/health/kidney-cancer/
Other Sites
https://www.vitals.com/doctors
This is a free web site for information about 700,000 practicing physicians in the United States.
https://www.apexmd.com/Default.aspx
Free web site for finding US Practitioners for named conditions. Search can be refined by area. Although HLRCC is not currently recognized, VHL is and many physicians cover both conditions. If you have searched by area, scroll down to the displayed information. Do not click on to any links as they will expand to the whole of the US. For example https://search.apexmd.com/search2.aspx?q=vhl&r=5 will show 9 urology physicians in Texas. Clicking on to the urology link will show all 1000 US physicians
https://formspal.com/health-support/
In US ” We Support Health by Providing Free Legal Forms Online” a useful website providing some of the most widely used online forms and documents include a medical power of attorney (POA), living will, do-not-resuscitate orders (DNR), and health care proxy. Each of these is crucial and an absolute must at various stages throughout life. More general free forms on all aspects of US living can be found at https://formspal.com
https://www.caringbridge.org
Has free patient websites to help family and friends share information and support. This is particularly helpful for people who are currently in the hospital or undergoing longer treatments.
https://www.orpha.net//consor/cgi-bin/index.php?lng=EN
The portal for rare diseases and orphan drugs in Europe
Various Addiction Resources
drug-rehabs.org
Mental Health & Addiction Resources Advocates for those struggling with addiction and dedicated to educating people about drug and alcohol abuse, as well as helping individuals who are seeking treatment. Provides resources for treatment programs in or near your area. Only lists treatment centers approved by Samhsa in an easily searchable state-by-state directory.
Addicted.org
Also known as Drug Rehab Services, is a family-owned business committed to helping individuals and their families across the United States find a drug rehab center that can help them overcome addiction and prevent substance use.
AddictionResource.com
A volunteer-run organization that focuses on providing accurate, reliable, and up-to-date information regarding substance addiction. There is also a specific website AlcoRehab for alcohol addiction, treatment and recovery.
alcoholrehabhelp.org
Alcohol Rehab Help is an informational web guide created for people in the U.S.A. struggling with alcohol use disorders (AUD) and co-occurring mental health disorders. Not only do we offer information on Alcohol Use Disorder, but we also have comprehensive information regarding treatment options.
These two Alcohol Rehab articles have connected many patients to recovery options: How Long Does It Take To Sober Up? Am I An Alcoholic?
New Directions for Women (NDFW) is based in US California and gives support for ALL Women Seeking Addiction Treatment with a rehab for women, with a model designed by women. Its directed approach caters to the variables women face in life and in treatment.
Quit Smoking Community
Quit Smoking Community is a volunteer-run organization that helps people wanting to stop smoking. Also on Facebook Page and Facebook Group.
Addiction Treatment Programs, Nationwide Rehab Centers That Fit Your Needs Find your nearest rehab center.
National Council on Seniors Drug & Alcohol Rehab – non-profit organization with a mission to educate and provide assistance to seniors struggling addiction as well as caregivers and family members with concerns. The primary objective is to effectively halt the growing silent epidemic of senior addiction.
You may be tempted to start Vaping as an alternative. Please read this article first Vaping 101 – Health Relation, Benefits, Dangers, Fun Facts, And More
healthfinder.gov
A US government website where you will find information and tools to help you and those you care about stay healthy.
Using Family Medical Leave Act (FMLA) To Go To Rehab
Making the decision to go to rehab is not easy. Considering all areas of life are affected, it may ease your mind to know that substance abuse treatment is included in the US Family Medical Leave Act, and that, in many cases, your job will be protected while you recover.
RxDangers.com
RxDangers.com aims to be your trusted resource, educating the US public about all defective medical devices and dangerous medications that are available on the market today.
Recall Report was created to alert the public to the latest information on dangerous drugs and products.
Cerebral Palsy Guidance and Cerebral Palsy Group
These sites may be of interest to our Fumarase Deficiency families as it has a lot of good information on developmental and intellectual disabilities, as well as information about emotional effects, counseling and more.
CLINICAL TRIALS
The list of clinical trials and studies is constantly changing and people are advised to seek out the latest information from your medical specialists or by contacting info@hlrccinfo.org. The following was current at the time of writing this document.
The Natural History Study at the National Institutes of Health
The US-NIH, currently has a Natural History study for individuals who have been diagnosed with HLRCC or who have the clinical symptoms that might imply a possible diagnosis.
If you have an interest in the US-NIH Study, contact:
Cris Leite
Patient Care Coordinator
NIH/NCI
Urologic Oncology Branch
10 Center Drive Rm. 2W 5750
Bethesda, MD 20892-1208
T:(240)858-3913
F:(301)435-9262
Email: Leitec@mail.nih.gov
or
Debbie Nielsen, BSN
Genetic Counselor
Urologic Oncology Branch
National Cancer Institute
National Institutes of Health
Bldg. 10, CRC, Rm. 2W-5740
9000 Rockville Pike
Bethesda MD 20892
T: (240) 760-6247
F: (301) 480-2869
Email: Deborah.Nielsen@nih.gov
For HLRCC drug trials, please contact
Erin N. Purcell, BSN, RN
Research Nurse Specialist
National Cancer Institute
National Institutes of Health
9000 Rockville Pike
Bethesda MD 20892
T: (240) 858-3933
F: (301) 480-2869
Email: erin.purcell@nih.gov
The US-NIH website: www.nih.gov
https://clinicaltrials.gov/ct/show/NCT00050752?order=2
https://clinicalstudies.info.nih.gov/detail/A_2003-C-0066.html
“Genetic Study of Cancer Risk and Gene Identification in Patients and Families With Hereditary Leiomyomatosis and Renal Cell Cancer Syndrome”
- This study is currently recruiting participants as of February 2013. The study is now seeing new people with HLRCC who have a kidney cyst or a solid tumor and also one new first person from a new family with HLRCC. Other people at risk in HLRCC families should be screened by their local medical centers. The Trial Number was NCT00055627 (now obsolete).
UCLA has created a registry to characterize the burden of HLRCC, determine who is at risk for skin, uterine, adrenal, and kidney manifestations, and help find new cures for this condition. Patients at other centers have successfully had their tumors sent in to make new models of HLRCC kidney cancer. Please contact them at kidneycancer@mednet.ucla.edu
Phase II Pamiparib and Temozolomide
https://clinicaltrials.gov/show/NCT04603365
“A Phase II Study of Pamiparib and Temozolomide for the Treatment of Hereditary Leiomyomatosis and Renal Cell Cancer”
Brief Summary:
This phase II trial investigates how well pamiparib and temozolomide work in treating patients with hereditary leiomyomatosis and renal cell (kidney) cancer. Poly adenosine diphosphate-ribose polymerase (PARPs) are proteins that help repair DNA mutations. PARP inhibitors, such as pamiparib, can keep PARP from working, so tumor cells can’t repair themselves, and they may stop growing. Chemotherapy drugs, such as temozolomide, work in different ways to stop the growth of tumor cells, either by killing the cells, by stopping them from dividing, or by stopping them from spreading. Giving pamiparib and temozolomide may help treat patients with hereditary leiomyomatosis and renal cell cancer.
Collaborators:
BeiGene www.beigene.com/
Driven To Cure www.driventocure.org/
Phase II Study of Bevacizumab and Erlotinib
https://clinicaltrials.gov/show/NCT01130519
“A Phase II Study of Bevacizumab and Erlotinib in Subjects With Advanced Hereditary Leiomyomatosis and Renal Cell Cancer (HLRCC) or Sporadic Papillary Renal Cell Cancer”
This clinical trial of bevacizumab (AVASTIN® | Genentech, Inc.) and erlotinib (Tarceva® is ongoing, and is again (May 7, 2015) recruiting patients with papillary kidney cancer that has spread (metastasized) beyond the kidneys. Very good interim results have been reported in https://medicalxpress.com/news/2014-11-kidney-cancer-patients-combination-anti-cancer.html Kidney cancer patients respond well to a combination of two existing anti-cancer drugs
In Annual Meeting News W. Marston Linehan, M.D is reported as saying:
“As for HLRCC syndrome, NCI began focusing on this familial kidney cancer syndrome in the 1980s. Researchers learned that these patients develop a particularly aggressive form of type 2 papillary kidney cancer. In addition to raised and painful cutaneous leiomyomas, 90 percent of female patients in these HLRCC syndrome families also develop uterine fibroids.”
“HLRCC is one of the most malignant types of kidney cancer there is,” Dr. Linehan said. “It needs to be detected because it can spread early and can be lethal.”
HLRCC syndrome is caused by an alteration of the Krebs cycle enzyme, fumarate hydratase. In studying this fumarate hydratase pathway in HLRCC, NCI researchers learned that when the fumarate hydratase gene in the cancer cell is damaged, it alters its metabolism significantly, becoming exceptionally dependent on glycolysis and glucose uptake.
“We have developed an approach to treatment that involves using bevacizumab and erlotinib, therapeutic agents that target the vulnerability of this fumarate hydratase pathway in HLRCC patients with advanced kidney cancer,” Dr. Linehan said. “This is currently an ongoing clinical trial, and we are cautiously optimistic about the early results.”
He also reported that blood tests are available to assist clinicians in making a diagnosis by detecting fumarate hydratase (FH) for HLRCC syndrome and folliculin (FLCN) for BHD syndrome.
“In both of these hereditary cancer syndromes, it is important for dermatologists and other clinicians to understand the significance of fibrofolliculomas and leiomyomas,” Dr. Linehan said. “These patients need to be evaluated for the possible presence of kidney cancer when they present with these dermatologic findings.” Listen to W. Marston Linehan, M.D (MP3)
Editor’s Note: Additional drugs will be forthcoming that will target the FH pathway. Stay tuned for more news.
Phase I/II Study of Vandetanib and Metformin
https://clinicaltrials.gov/ct2/show/NCT02495103
“Vandetanib in Combination With Metformin in People With HLRCC or SDH-Associated Kidney Cancer or Sporadic Papillary Renal Cell Carcinoma”
This Phase I/II clinical trial of vandetanib (CAPRELSA® | AstraZeneca United States ) and metformin is ongoing, and recruiting (July, 2015) patients with papillary kidney cancer that has spread (metastasized) beyond the kidneys.
Phase II Trial of the DNA Methyl Transferase Inhibitor Guadecitabine (SGI-110)
https://clinicaltrials.gov/ct2/show/NCT03165721
A Phase II Trial of the DNA Methyl Transferase Inhibitor, Guadecitabine (SGI-110), in Children and Adults With Wild Type GIST,Pheochromocytoma and Paraganglioma Associated With Succinate Dehydrogenase Deficiency and HLRCC-associated Kidney Cancer
Wild-type gastrointestinal stromal tumor (GIST) is a cancer in the esophagus, stomach, or intestines. It does not respond well to standard chemotherapy or radiation therapy. Most people with GIST are treated with imatinib. But it may not work in many children with GIST. Researchers think the drug SGI-110 may help treat people with GIST, pheochromocytoma and paraganglioma (PHEO/PGL), or kidney cancer related to hereditary leiomyomatosis and renal cell carcinoma (HLRCC).
Phase I Study of the Glutaminase Inhibitor CB-839 in Solid Tumors
https://clinicaltrials.gov/ct2/show/NCT02071862
This phase I trial using CB-839 is recruiting (December, 2015) patients with Fumarate Hydratase (FH)-deficient tumors.
Phase 2 Trial Olaparib with and without AZD1775, AZD5363, and AZD2014 in Treating Patients with Advanced Solid Tumors
https://clinicaltrials.gov/ct2/show/NCT02576444
Researchers at Yale have just opened a clinical trial that they believe specifically addresses the underlying biology of HLRCC. (They are actively looking for HLRCC patients at this time). Their description in lay language: Cancer patients with a family history of FH or SDH mutations, or tumors found to have these mutations. These mutations most typically appear in patients with hereditary kidney cancers including syndromes such as HLRCC. Genetic testing must have been completed that confirms the presence of this mutation. For patients with a history of HLRCC, the investigators at Yale can assist with confirmation of the mutation in the tumor(s). HOW do I get more information? Contact ranjit.bindra@yale.edu or brian.shuch@yale.edu
There is more information in a conversation in Smart Patients.
Treatment of Cutaneous Leiomyomas with Botulinum Toxin
https://clinicaltrials.gov/show/NCT00971620 “Randomized Pilot Study for the Treatment of Cutaneous Leiomyomas with Botulinum Toxin”
This study is ongoing, but no longer recruiting participants.
This NIH study has published a result “The use of botulinum toxin to treat painful cutaneous leiomyomas was associated with improved quality of life and with a trend toward improved pain at rest.” Efficacy of Intralesional Botulinum Toxin A for Treatment of Painful Cutaneous Leiomyomas: A Randomized Clinical Trial.
Intravenous Recombinant Human IL-15
https://www.clinicaltrials.gov/ct2/show/NCT01021059
“A Phase I Study of Intravenous Recombinant Human IL-15 in Adults With Refractory Metastatic Malignant Melanoma and Metastatic Renal Cell Cancer”
This study has completed. No results yet published.
EXTENSIVE LIST OF RELEVANT RESEARCH ARTICLES
Please refer to our separate “HLRCC Science” document
BACKGROUND of the TERM “HLRCC”
Since the 1950s some benign skin lumps were known to be inherited in some families and the cells have a distinctive appearance under a microscope see Hereditary Multiple Leiomyoma of The Skin, Warner et al. 1958
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1931875/
Full text
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1931875/pdf/ajhg00572-0055.pdf
However, the term “myoma” was defined a hundred years before by Virchow in 1854.
The lumps were termed “cutaneous leiomyomas”, “cutaneous piloleiomyomas” or “cutaneous pilar leiomyomas”. These are benign smooth muscle tumors arising from the arrectores pilorum (singular: arrector pili) muscles associated with the hair follicles of the skin.
Cutaneous leiomyomas are made up of a poorly circumscribed proliferation of haphazardly arranged smooth muscle fibers located in the dermis that appear to infiltrate the surrounding tissue and may extend into the subcutis.
The term “multiple cutaneous leiomyoma” (MCL) was used when several lumps were present. They occur in clusters or singly on arms, legs, and trunk and sometimes on the face. There is a classification of Type 1 for solitary and Type 2 for multiple in cluster patterns. It was then noted by W.B. Reed et al. in a published paper in 1973 that females with this condition also invariably had uterine leiomyomas (fibroids).
The term Reed’s Syndrome or “multiple cutaneous and uterine leiomyomas” (MCUL) was then used to describe this condition. MCL and MCUL are defined in the definition of HLRCC in the Online Mendelian Inheritance in Man (OMIM): https://www.ncbi.nlm.nih.gov/omim/150800
It was nearly 30 years later in 2001 that V. Launonen et al. published a paper linking malignant kidney cancer to the syndrome. This was a major advance from a relatively benign condition to a much more serious possibility of malignant cancer and the term “hereditary leiomyomatosis and renal cell cancer” (HLRCC) was used to describe the condition when kidney cancer was present. HLRCC is defined in MIM ID #605839
https://www.ncbi.nlm.nih.gov/omim/605839
In 2002 I.P. Tomlinson et al. identified alterations in the FH gene as being responsible.
To date there are over a 100 different FH gene alterations described in a genetic database.
https://www.biomedcentral.com/1471-2350/9/20
Unfortunately, all these terms are in use to relate to the one condition – MCL, MCUL, MCUL1, Reed’s or Reed Syndrome, HLRCC, LRCC, Fumarate Hydratase (FH) Gene Alteration and Fumarase. This makes searching for information on the Internet very difficult. The acronym HLRCC is not always present to help the search. Some dermatologists persist in using Reed’s Syndrome despite the fact that it is not used for the OMIM 150800. Also do not be confused by a completely unrelated condition called Familial Hypercholesterolemia (abbreviated FH or Fh) which although genetic is caused by completely different genes – LDLR, APOB, and PCSK9 genes.
There is further opportunity for misunderstanding in that the Fumarate Hydratase (FH) Gene Alteration is responsible for two distinct conditions. (1) HLRCC and (2) Fumarase Deficiency.
This handbook is mainly concerned with hereditary leiomyomatosis and renal cell cancer – caused by single alterations in the FH gene. There is a separate section on Fumarase Deficiency.
In 2023 over 1000 alterations in the FH gene that may cause hereditary leiomyomatosis and renal cell cancer (HLRCC) have now been reported in ClinVar. Most of these alterations replace one amino acid with another amino acid in the fumarase enzyme. The 1000+ alterations are classified as pathogenic (265), likely pathogenic(143), and variants of unknown significance VUS(650). The VUS figure shows the importance of reporting HLRCC symptoms against variants to improve classification
People with HLRCC are born with one altered copy of the FH gene in each cell. The second copy of the FH gene in certain cells may also acquire alterations as a result of environmental factors such as ultraviolet radiation from the sun or a mistake that occurs as DNA copies itself during cell division. These changes are called somatic mutations and are not inherited.
FH gene alterations interfere with the enzyme’s role in the citric acid cycle, resulting in a buildup of fumarate. Researchers believe that excess fumarate may interfere with the oxygen level detection system in the cell. Stabilization of hypoxia inducible factor (HIF) due to pseudohypoxia (false indication of low oxygen even when oxygen is plentiful) in cells with two altered copies of the FH gene may encourage tumor formation and result in the tendency to develop leiomyomas and renal cell cancer.”
MIM ID *136850 describes the FH gene in https://www.ncbi.nlm.nih.gov/omim/136850
Another way to have HLRCC without inheriting an FH variant is through a process known as somatic mosaicism. Very early on in the development of a embryo (baby), one of its cells can randomly acquire a mutation in its FH gene. As this cell continues to divide, every cell that descends from that originals cells lineage will also contain that mutation. This creates a scenario in the body where there are now two genetically distinct populations of cells; some with normal DNA, and some with the new FH variant. Depending on which tissues of the body these mosasic cells end up in will determine they are at risk to develope HLRCC-associated tumors. An individual with somatic mosaicism may not always test positive with genetic screening. This happens if their blood or salvia does not have cells containing the FH variant. Also, if their sperm or egg cells do not contain the FH variant, their children cannot inherit HLRCC.
FUMARASE DEFICIENCY
Happens when BOTH parents have an FH alteration
|
|
Parent 2 with HLRCC |
Each child gets one copy of the FH gene from each parent.
In this way, there are four possible arrangements of these four genes. Each arrangement has a 25% chance.
So there is a 50% chance of having HLRCC and a 25% chance of having fumarase deficiency and a 25% of not having either condition.

AC: Child |
AD: Child |
BC: Child |
BD: Child |
Shown here is a 25% chance of developing Fumarase Deficiency based on both parents having a FH alteration. Fumarase Deficiency is a Autosomal Recessive condition as it requires both genes to have alterations (though not necessarily the same alteration).
For more information https://www.nlm.nih.gov/medlineplus/ency/article/002049.htm
From Genetics Home Reference: https://ghr.nlm.nih.gov/gene/FH
fumarase deficiency – caused by alterations in the FH gene usually from both parents. It is also known by the name of fumaric aciduria.
Approximately 17 FH gene alterations that cause fumarase deficiency have been reported. However many (if not all) FH gene alterations probably have the potential to cause this condition but are not seen because they would be incompatible with fetal life. Fumarase deficiency occurs in individuals who inherit two altered copies of the FH gene in each cell. (This is different from HLRCC, in which individuals have one altered copy and one normal copy of FH in each cell). In fumarase deficiency, most of these alterations replace one protein building block (amino acid) with another amino acid in the fumarase enzyme. These changes disrupt the ability of the enzyme to help convert fumarate to malate, interfering with the function of this reaction in the citric acid cycle. Impairment of the process that generates energy for cells is particularly harmful to cells in the developing brain, and this impairment results in the signs and symptoms of fumarase deficiency (also known as fumaricaciduria). This is defined in MIM ID #606812.
There is one specific FH variant that is commonly found to be a contributor in Fumarase Deficiency. Namely, FH c.1431_1433dupAAA (p.Lys477dup). Despite being classified as a pathogenic variant, carriers of this variant are not known to have an increased risk for developing kidney cancer (see paper by Zhang 2020). This is in marked contrast to other FH variants. Because of its lack of association with renal cancer, this variant is currently classified as a Variant of Unknown Significance (VUS) for HLRCC. People who carry this variant should still be aware that they can potentially cause Fumarase Deficiency in their offspring. If the other parent is also carrier a dysfunctional FH gene, any child conceived will have a 25% risk of inheriting Fumarase Deficiency. As a precaution, genetic testing of the other parent is advised to make sure no other FH variant is present.
https://www.ncbi.nlm.nih.gov/omim/606812. Fumarase deficiency has had widespread publicity because of its polygamy connections see www.childbrides.org/taxes_PNT_forbidden_fruit.html
Symptoms and Diagnosis
The condition has considerable variation from relatively mild symptoms to very severe leading to an early death. The new born baby has brain defects leading to seizures and doesn’t develop normally. There may be a distinctive facial appearance. This link https://rarediseases.info.nih.gov/GARD/Condition/6476/QnA/37149/Fumarase_deficiency.aspx provides a more comprehensive description. A high level of fumaric acid level in the urine is a key indicator. MRI scans of the brain can be used to see the extent of malformation. A genetic test to determine the FH gene alterations is the definitive test. The parents would also be tested for FH gene alteration as they would normally each have the HLRCC condition.
Treatment and Management
There is no cure for fumarase deficiency and treatment is attending to the conditions symptomatically to prevent further harm, as in the case of seizures. Depending on severity suitable diets may help with feeding difficulties and a wheelchair to provide physical support may be useful. This link Lacosamide-Responsive Status Epilepticus And Epileptic Spams In Fumarase Deficiency (P2.186) gives a case study of successful treatment for the epileptic symptom using lacosamide after other treatments had failed.
HOW DO CHANGES IN DNA CAUSE CHANGES IN FUMARASE?
If your genetic test results show that you have an alteration in your fumarase gene, you may have questions about what the letters, numbers, and symbols that describe the alteration mean. You may also wonder how changes in the DNA of your fumarase gene interfere with the making of fumarase in your cells.

Krebs Cycle

The Krebs Cycle was discovered by Hans A. Krebs. It takes place in the innermost space of the mitochondria and requires the presence of oxygen. Together with the electron transport chain, it produces most of the cells’ energy.
GLOSSARY: Definitions of Commonly Used HLRCC Terms
Assay – Used to measure the quantity of fumarase enzyme in a sample of skin cells.
Autosomal – when the gene defect is located on one of the 22 regular chromosomes and not on a sex chromosome (X or Y). The result is that males and females may have the condition, in approximately equal numbers.
Citric Acid Cycle – see Krebs Cycle.
CT Scan – Computed Tomography also known as CAT (Computerized Axial Tomography) uses a computer to combine many x-ray images to generate cross-sectional views and 3-dimensional images of internal organs and structures of the body.
Cutaneous – Pertaining to the skin – not only the skin surface, but also in the skin layers.
Dominant – a gene is dominant when it is only necessary to have one altered copy of the gene in order to have the condition. Consequently, if the gene is autosomal (on a chromosome other than the X or Y chromosome), there is a 50% chance of a child inheriting the condition.
FH – Fumarate Hydratase, the enzyme encoded by the gene associated with HLRCC
Fibroid – is a benign (non-cancerous) tumor that originates from the smooth muscle layer of the uterus and its connective tissue. It is a uterine leiomyoma.
Fumarase – (or fumarate hydratase) is an enzyme that catalyzes the reversible hydration/dehydration of Fumarate to S-malate in the Krebs Cycle.
Fumarate – This chemical is formed during the basic cell energy cycle known as the Citric Acid Cycle or Krebs Cycle.
Genotype – This is the specific genetic information of the cells in your body.
HLRCC – Hereditary Leiomyomatosis and Renal Cell Cancer.
Hereditary – passed from one generation to the next.
Krebs Cycle – is a series of chemical reactions which is used by all aerobic living organisms to generate energy through the oxidization of acetate derived from carbohydrates, fats and proteins into carbon dioxide and water.
Leiomyoma – an abnormal growth of smooth muscle tissue. In HLRCC there are cutaneous and uterine leiomyoma.
Leiomyomata – the correct Latin plural form of leiomyoma. However most articles now use leiomyomas instead.
Leiomyomatosis – means the occurrence of leiomyomas in the body.
LOH – Loss of Heterozygosity – HLRCC tumors are found to have no fumarase activity, which is termed Loss of Heterozygosity (LOH) for FH. The two alleles of the FH gene were different (one altered) but now they are both altered. This represents the “second hit” to FH gene function in this one cell, the loss of the normal function of the second copy of the FH gene through somatic alteration.
Metastasize – when cancerous cells break off from the primary tumor and travel to other parts of the body and start new secondary tumors.
MRI Scan – Magnetic resonance imaging, a type of scan that uses no ionizing radiation. It provides a good contrast between the different soft tissues of the body. Gadolinium contrast is used to enhance the 3d-image.
PET/CT Scan – Positron Emission Tomography (PET) combined with an x-ray Computed Tomography (CT) is used to trace glucose metabolism (using fluorodeoxyglucose, FDG). High uptake is seen in HLRCC tumors. https://www.radiologyinfo.org/en/info.cfm?pg=pet.
Phenotype – These are the actual observed symptoms that you have which researchers try to match to your genetic alteration – see Genotype.
Piloleiomyoma – the full name of the benign skin lump, sometimes preceded by the word “cutaneous” or shortened to just “leiomyoma”
Primary Tumor – a tumor which has developed in its original place, grown from a single cell.
Progress – to continue to get worse, a term used for cancer which has worsened, such as increased tumor size or cancer spread.
Recessive – a gene is recessive when it is necessary to have two altered copies of the gene in order to have the condition (though not necessarily the same alteration).
Remission – used in conjunction with the words “complete” and “partial”. Complete remission is no sign of any remaining cancer. Partial remission is an improvement, tumor shrinkage or less activity etc.
Clear cell Renal Cell Carcinoma (RCC) – is the most common type of kidney cancer in adults (carcinoma = a type of cancer).
RCC Classification – In the general population kidney cancer accounts for about 1-2% of all cancers. Renal Cell Carcinoma(RCC) is divided into groups : Clear cell, Papillary, Oncocytic and Chromophobe, Collecting Duct, Other Renal, Molecularly Defined. In Molecularly Defined there is Fumarate Hydratase-deficient renal cell carcinoma which includes RCC associated with HLRCC and also sporadic cases.
Scan Types – There are several different types of scan – See entries for MRI, CT, PET/CT, Ultrasound, and Bone.
TCA – tricarboxylic acid cycle see Krebs Cycle.
Ultrasound Scan – An ultrasound scan is a painless test that uses sound waves to create images of organs and structures inside your body. It can be used on kidneys, but there is a risk that not all tumors will be detected. In HLRCC it can be useful to track fibroids in the uterus.
HANDOUTS for PRINTING
On the following pages is a separate small document which can be modified for your own use:
You might also consider printing our HLRCC Quick Facts (Printable) and HLRCC Brochure.
Family Letter (to send to relatives of someone recently diagnosed with HLRCC)
To Members of the ___________ Family,
I hope this letter finds all of you happy and in good health. My main reason for writing this is to inform my relatives of a hereditary medical condition that I have been diagnosed with. The condition is extremely rare in the general population, but it runs in families. Since I have it, this means that others in the family are at risks up to 50%. It is called Hereditary Leiomyomatosis and Renal Cell Cancer (HLRCC). The kidney cancer component of this disease can be fatal if not treated in time.
I am hoping that you will act on this information since this is a hereditary condition. We all have a risk as high as 50% of having the gene alteration. If we have it, our children have a 50% chance of having it (and so on). Consequently, some members of a particular branch of the family may have members with the condition while others are free of it. Having a genetic test is the best way to be diagnosed with the condition. Even if you decide not to be genetically tested I encourage you to seek screening advice, actions you can take to watch for signs of trouble.
People with this condition are susceptible to the development of the following:
- Uterine Fibroids in females, often early onset, multiple, large and symptomatic, usually detected in the 20’s and 30’s, may impact the ability to have children, and often lead to hysterectomy.
- Skin Leiomyomas (non-cancerous growth) of the skin, usually on the stomach, back, arms and legs, can be isolated or clustered lesions or can be disseminated (segmental), sometimes painful or may not hurt, and typically onset is in 30’s but have been seen in children. They usually appear as small firm, pink raised growths (sometimes white) or bumps in clusters and are difficult to diagnose yourself: https://www.dermnet.com/Leiomyomata/photos/1
- Kidney Cancer – individual risk is not completely known at this time, but a high percentage of adults with this condition have been found to have kidney tumors. The average age of symptomatic kidney cancer is 44, but we think that survival is better when tumors are found before symptoms occur. Even children have been diagnosed with this type of kidney cancer
Those with HLRCC need to be screened annually for kidney tumors, preferably by a thin-sliced MRI with contrast. Even small tumors have been known to metastasize (spread) so annual screening is the very best way to catch tumors as early as possible.
The HLRCC Foundation is a strong organization that can help address your questions and concerns. Go to https://www.hlrccinfo.org to access a detailed handbook and to join the support group. You can also find information about a large on-going study at the National Institutes of Health (US-NIH) that you may be able to participate in should you test positive for HLRCC.
Please call me at _____________________ to discuss this letter further. You can also call their toll free number:
1-800-767-4845 ext. 709 or +1-617-277-5667 ext. 709
or write to:
HLRCC Foundation c/o VHLFA,
2001 Beacon Street,
Suite 208, Boston,
MA 02135
USA
Love to you all.

Last Updated on 7th February 2025 by Graham


